TallGuyJohninBKK
-
Posts
37,162 -
Joined
-
Last visited
-
Days Won
6
Content Type
Events
Forums
Downloads
Quizzes
Gallery
Blogs
Everything posted by TallGuyJohninBKK
-
 "For the second wave since April, Zhong’s modeling revealed that the XBB variant is expected to cause 40 million infections weekly by May, going up to 65 million in June. This goes against the grain of Chinese health officials’ estimate that the wave had peaked in April. In Beijing, the number of new infections recorded between May 15 and 21 grew four times in four weeks." And, in one illustration of how government policies increasingly are making COVID data reporting unreliable on the undercounting side, virtually none of those Chinese COVID cases are officially being reported by China to the World Health Organization for use in their global COVID tallies.... Just like Thailand last fall stopped actually publicly counting and reporting COVID infections / positive tests, and now only reports COVID hospitalizations as "cases."
"For the second wave since April, Zhong’s modeling revealed that the XBB variant is expected to cause 40 million infections weekly by May, going up to 65 million in June. This goes against the grain of Chinese health officials’ estimate that the wave had peaked in April. In Beijing, the number of new infections recorded between May 15 and 21 grew four times in four weeks." And, in one illustration of how government policies increasingly are making COVID data reporting unreliable on the undercounting side, virtually none of those Chinese COVID cases are officially being reported by China to the World Health Organization for use in their global COVID tallies.... Just like Thailand last fall stopped actually publicly counting and reporting COVID infections / positive tests, and now only reports COVID hospitalizations as "cases." -
COVID vaccinations don't cause COVID. Perhaps you should look at your own behaviors, as to why you supposedly kept coming down with the virus, when others such as myself didn't. "MYTH: A COVID-19 vaccine can make me sick with COVID-19. FACT: Because none of the authorized COVID-19 vaccines in the United States contain the live virus that causes COVID-19, the vaccine cannot make you sick with COVID-19." https://www.cdc.gov/coronavirus/2019-ncov/vaccines/facts.html "Myth: You can get COVID-19 from the vaccines. This is FALSE. “There’s no live virus in the vaccines, so they can’t infect you,” says Dr. Cunningham. “Basically, the vaccines make our bodies produce one single protein from the virus—the protein that infects our cells. By making that protein, we prevent infection. You might have side effects like a headache or chills, but that’s because your body is creating an immune response, not because you have an infection.” https://www.henryford.com/blog/2021/08/vaccine-myths
-
The time is greater now than any time thus far in 2023: Thailand weekly new COVID hospitalizations and deaths: March 26 to April 1: May 21 to 27: https://www.facebook.com/informationcovid19/posts/pfbid02tXUeEnaX7KySm7i7jAyPCUYaMemoQEPccFeAgjfANwb55nUWFzRphFuHWPp1o99Cl -- New weekly COVID hospitalizations in Thailand (2,970) are at the highest level thus far for 2023. --COVID patients hospitalized in serious condition (425) are at the highest level thus far for 2023. --COVID hospitalized patients requiring intubation in order to breathe (253) are at the highest level thus far for 2023.

-
Reputable studies, and organizations such as the U.S. National Institutes of Health, have found insufficient evidence that Vitamin D actually helps prevent or treats COVID. Vitamin D doesn't prevent COVID-19, other respiratory infections, studies find https://www.cidrap.umn.edu/covid-19/vitamin-d-doesnt-prevent-covid-19-other-respiratory-infections-studies-find AND "NIH COVID-19 Treatment Guidelines Although multiple observational cohort studies suggest that people with low vitamin D levels are at increased risk of SARS-CoV-2 infection and worse clinical outcomes after infection (e.g., higher mortality rates), clear evidence that vitamin D supplementation provides protection against infection or improves outcomes in patients with COVID-19 is still lacking.1,2 Recommendation There is insufficient evidence for the Panel to recommend either for or against the use of vitamin D for the prevention or treatment of COVID-19." https://www.covid19treatmentguidelines.nih.gov/therapies/supplements/vitamin-d/ As the NIH document above explains, the various studies that have found benefit from Vitamin D tend to have been poorly done or have other limitations that make their findings suspect.
-
Perhaps that's because... --In Thailand, new COVID hospitalizations are at a year-high level for 2023, more than 400 new per day on average, and have been steadily rising since April. --Whereas in the U.S. for example, COVID cases, hospitalizations and deaths have been declining pretty steadily for months now. Some people here seem to have geographic confusion... This is Thailand, not the U.S. or the U.K. The COVID situation here should be judged on what's occurring here...not in some other countries with entirely different COVID situations. Back in March when new COVID hospitalizations in Thailand were running 150-170 per week, no one was much talking about COVID here, myself included. But now, new COVID hospitalizations in Thailand have steadily risen for the past two months to now nearly 3,000 per week, and people are rightfully talking.
-
No, you take the Thai Ministry of Public Health's word for it, when they count them as "COVID deaths" and "COVID hospitalizations."
-
The source is the Thai Ministry of Public Health, which compiles and reports the COVID deaths and hospitalizations data. If you don't believe them, I'm sure they'd be happy to hear from you.
-
The vaccines DO prevent infections, just not 100%. More earlier in the pandemic. Less more recently amid Omicron. That's absolutely true. As for your quoted comments, you mean to tell me politicians mis-speak? Really! Surely, it's never happened before.
-
Thailand doesn't follow the same reporting rules as the UK, nor does the U.S. for that matter. And the UK had different COVID death counting policies among different agencies. Read again what I wrote above regarding Thailand. It was clear and specific as to what are reflected in Thailand's COVID death statistics, though I don't have a breakdown for the shares of deaths with COVID as the main cause vs. COVID as a contributing cause. Background on the UK: "Claims that COVID-19 deaths are lower than reported have been common throughout the pandemic from critics who argue the virus is not as serious as we are being led to believe. In fact, however, researchers have found evidence that overall deaths from COVID-19 have been undercounted, not overcounted, since the start of the pandemic." https://www.politifact.com/factchecks/2022/jan/24/youtube-videos/no-death-totals-covid-19-england-have-not-been-ove/
-
Thailand counts them as COVID deaths, which under their system, means the death was either caused by COVID or COVID was a contributing factor.
-
Yes they are, but not as effective as they had been against prior variants. No, that isn't "best." Thailand had nearly 3,000 new COVID hospitalizations in the past week, a new weekly high for 2023, and 42 new COVID deaths. Don't wish for the pandemic here to get any worse than it already is.
-
It was a tiny blip on what now is a 3-1/2 year long COVID pandemic. If her comments encouraged more people to get vaccinated and thus in reality actually ended up reducing their chances of getting sick from or dying from COVID, thus saving lives, I'll forgive her the momentary, one-off misspeak.
-
What vaccines have been able to do against the COVID virus have changed regularly since the outbreak of the pandemic right up thru today, not because public figures were intentionally misleading, but because the virus has evolved and mutated into new and different forms -- Alpha, Delta, Omicron, etc. At the very beginning of the pandemic, the research was clear at that time, against the original version of the virus, that the mRNA vaccines had a very high impact in preventing infections. But that didn't last as the pandemic continued and the virus mutated. Pfizer and BioNTech Conclude Phase 3 Study of COVID-19 Vaccine Candidate, Meeting All Primary Efficacy Endpoints Wednesday, November 18, 2020 "Primary efficacy analysis demonstrates BNT162b2 to be 95% effective against COVID-19 beginning 28 days after the first dose... ... Efficacy was consistent across age, gender, race and ethnicity demographics; observed efficacy in adults over 65 years of age was over 94%" https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-conclude-phase-3-study-covid-19-vaccine
-
I don't believe there's any or much credible evidence that prior COVID infections will result in "long term" immunity, depending on how one defines the term "long term." The COVID virus keeps mutating, and as it does, the protections from past infections both diminish with passing time and diminish as the newer variants diverge more from the ones a person may have been infected with in the past. One of the largest reviews of the issue found that newer Omicron variants do a better job of evading immunity from prior infections, with the protection rate being only 36.1% for Omicron BA.1 at 40 weeks. "They found previous infection was highly protective against reinfection with alpha, beta and delta variants, but less so against omicron BA.1. A previous infection provided moderate protection from reinfection with omicron BA.1 (45 percent), compared with stronger protection against pre-omicron variants (82 percent). "Data from long-term studies showed that protection against reinfection for pre-omicron variants dropped to 78.6 percent over 40 weeks, whereas for omicron BA.1 it dropped more rapidly to 36.1 percent." https://www.sciencealert.com/largest-study-of-its-kind-shows-how-long-immunity-really-lasts-after-covid-infection It's not like a past COVID infection is some kind of permanent get out of COVID jail card.
-
Yes, she overstated the research that was known at that time, which later changed as the virus and science's understanding about it both evolved with time. Also, what she had said in the interview back in early 2021 was quickly corrected/clarified by her own agency. From the article you quoted: "Dr. Walensky spoke broadly during this interview,” a CDC spokesperson told the Times. “It’s possible that some people who are fully vaccinated could get Covid-19. The evidence isn’t clear whether they can spread the virus to others. We are continuing to evaluate the evidence.” None of that from early 2021 changes the reasons people then and now should keep current with their COVID vaccinations as recommended by public health agencies -- to reduce their risk of becoming infected, and even moreso, to even more substantially reduce their chances of becoming seriously ill or dying from COVID.
-
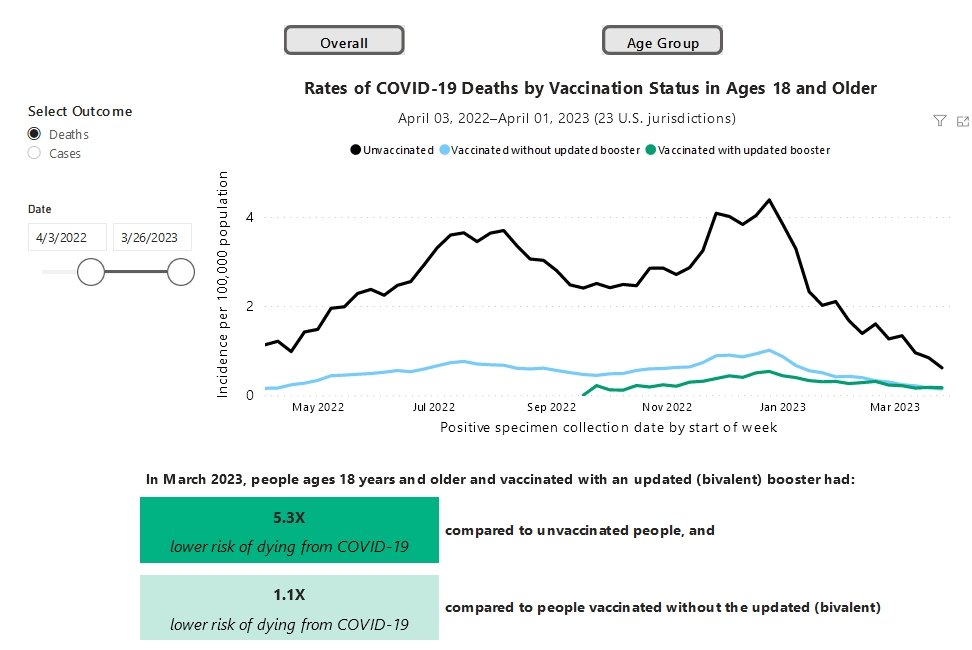
The difference is, the unvaccinated folks, overall, get sick and die from COVID at much greater rates than do the vaccinated, as numerous studies have documented, even during the recent Omicron period. https://covid.cdc.gov/covid-data-tracker/#rates-by-vaccine-status The CDC found that in March 2023, adults who had been vaccinated with the newer bivalent vaccines had a 5.3 times lower risk of dying from COVID than the unvaccinated.
-
COVID vaccines substantially REDUCE the risk of getting seriously ill or dying from COVID compared to being unvaccinated. If you haven't seen info regarding that, then you haven't been paying attention. From the U.S. CDC as of a week ago: "The VISION Network* assessed VE [vaccine effectiveness] against COVID-19–associated hospitalizations by time since bivalent vaccine receipt during September 13, 2022–April 21, 2023, among adults aged ≥18 years with and without immunocompromising conditions. During the first 7–59 days after vaccination, compared with no vaccination, VE for receipt of a bivalent vaccine dose among adults aged ≥18 years was 62% (95% CI = 57%–67%) among adults without immunocompromising conditions." "Among adults without immunocompromising conditions, VE [against COVID hospitalization] declined to 24% (95% CI = 12%–33%) among those aged ≥18 years by 120–179 days after vaccination." "VE against critical illness was 69% during the 7–59 days after receipt of a bivalent dose and was more sustained (50% at 120–179 days after bivalent vaccination) than VE against hospitalization." https://www.cdc.gov/mmwr/volumes/72/wr/mm7221a3.htm
-
As I said, the UK plans to continue offering COVID vaccines to those in the higher risk groups on a seasonal basis. Per your quoted document above: "Should a person move into an at-risk group, the offer of a first or second dose will re-open with the seasonal booster programmes." And elsewhere from the NHS: "After 30 June 2023 If you are eligible for a spring vaccination, or if you haven’t had your 1st or 2nd dose, the last date you will be able to get vaccinated is 30 June. After this date, you will only be eligible for a 1st or 2nd dose if you are at increased risk from COVID-19 and in most cases, you will have to wait until the autumn to get these vaccinations. If you develop a new health condition or start treatment that severely weakens your immune system, an exception may be made if your clinician advises you to get vaccinated sooner." https://www.england.nhs.uk/who-is-at-increased-risk-from-covid-19/ The UK isn't getting out of the COVID vaccines venture, just scaling it back.
-
I'm not a Brit. But from everything I've read, COVID vaccines are likely to continue being offered by the government in the UK to those in the older age groups who are most at risk... such as... the ages of a lot of the retired posters here.
-
The bivalent vaccines are (and have been available for some time) at multiple locations around BKK, and supposedly at select locations in other provinces.
-
yes... all of my recent past online submissions to BKK CW were typically having a 3 business day turnaround time.
-
Ya, except for the dead and hospitalized folks still being done in by COVID.... Their lives are hardly returning to normal. The latest MoPH weekly update says Thailand is currently averaging 424 new COVID hospitalizations per day.
-
Yes, that many people here continue to ignore commonsense COVID precautions at a time when new weekly COVID hospitalizations in Thailand just hit another new high for 2023.
-
Thanks much for the above answers to my question! ????
-
If I recall right, Thailand seems to have gotten most or all of its stock of bivalent COVID vaccines via donations from South Korea and France.... I don't believe I've seen anything indicating Thailand has, on its own, used its own money to buy stocks of the bivalent vaccines. Which is probably one reason why they're continuing to use/offer the older monovalent vaccine versions alongside the bivalent ones.