

partington
-
Posts
2,195 -
Joined
-
Last visited
Content Type
Events
Forums
Downloads
Quizzes
Gallery
Blogs
Posts posted by partington
-
-
58 minutes ago, ArcticFox said:
I keep hearing this too, but I never see the studies backing that assertion. All we hear are 'experts' who tell the public to trust them. My trust in government ran out decades ago. I want to see studies, data, and hard facts.
Now regarding the statement "Unvaccinated people are pools for the virus to mutate." This animal study shows it's probably the other way around, i.e., Vaccinated people are likely the source of virus mutation.
According to the study, vaccinated people are pools for the virus to mutate - IF - the vaccination does not convey full immunity. And guess what? None of the current crop of Covid vaccines provide the recipient with full immunity.
So the commonly accepted narrative being floated out by politicians and the press is that the unvaccinated are creating mutants that creates severe disease in the vaccinated.
This study shows the opposite to be true: "Our data show that anti-disease vaccines that do not prevent transmission can create conditions that promote the emergence of pathogen strains that cause more severe disease in unvaccinated hosts."
This is the exact opposite of what is being said by presidents, PMs, and high-level health care bureaucrats.
The former is a political statement; the latter is a scientific observation backed by research and analysis.
https://journals.plos.org/plosbiology/article?id=10.1371/journal.pbio.1002198This paper does not talk about "full immunity" - this is a term you seem to have pulled out of thin air.
It talks about vaccines which do not prevent transmission of the pathogen - termed 'leaky' vaccines - , and it specifically talks about the effect of leaky vaccines after hyperpathogenic (fatal) strains of a virus have emerged.
It does NOT say that leaky vaccines created the hyperpathogenic strains that kill the host nor that vaccination was responsible. Here is a direct quote:
"Our data do not demonstrate that vaccination was responsible for the evolution of hyperpathogenic strains of MDV, and we may never know for sure why they evolved in the first place."
What the paper ACTUALLY says is that IF a hyperpathogenic (fatal) strain develops then a leaky vaccine can promote the survival of that strain because it will prevent the death of those infected long enough for the fatal strain to be passed on. Normally a fatal strain dies out because it kills the host before transmission can occur.
Vaccines prevent death, in other words. But this is one of the major reasons we vaccinate people-to save their lives.
You have evidently missed the point that this presents a danger only to unvaccinated people and is therefore an additional argument for prompt population-wide mass vaccination, exactly as is done for smallpox say.
-
 2
2
-
-
More nonsense from you. This "study" includes results which are not statistically significant, that is they do not prove what they claim to and are therefore meaningless.
ALL reputable meta-analyses automatically exclude not statistically significant studies, because the definition of a study that is not significant statistically is that it has proved nothing.
This is not science. This is emotionally motivated lobbying, and is interesting only for the light it sheds on human psychology rather than disease treatment.
-
1
-
 1
1
-
-
- Popular Post
- Popular Post
5 hours ago, internationalism said:sinovac is inactivated, similar to astra.
thailand has approved mixing them when it transpired, that sinovac is ineffective against delta.
Now it also looks like astra is not good against delta as expected.
pfizer is mrna, different technology.
Mixing and matching is the best way of protection against different strains
For god's sake! The Astra Zeneca vaccine is NOT an inactivated SARS-CoV-2 vaccine, and has no similarities at all with the Sinovac vaccine.
The Astra vaccine is an adenovirus causing cells to express the spike protein of the SARS-CoV-2, which then acts as the antigen that the immune system detects and raises antibodies to.
The Sinovac vaccine is a preparation of the whole SARS-CoV-2 virus, which is inactivated and injected as the antigen.
They are completely different in every respect.
Be accurate!
-
3
-
1
-
- Popular Post
- Popular Post
5 hours ago, Boedog said:The pcr test or antigen test does not differentiate between Covid and the flu, it certainly does not define delta variant, you need a blood test for that, not long they will come up with another variant
This is simply wrong. The PCR test absolutely DOES distinguish between Covid and the flu.[ It is true that the routine test does not distinguish between Covid variants]
The reagents used in PCR tests are uniquely specific to the SARS CoV-2 coronavirus that causes Covid, because they contain nucleotide sequences that are absolutely unique to that virus. They are even able to differentiate between SARS-CoV-2 and other very closely related coronaviruses.
Flu is not even caused by a coronavirus, so is not detected by specific Covid-19 PCR tests at all.
Here is the US CDC explanation, which is, needless to say more reliable than non-factual random posts. Notice the paragraph at the end where the cdc describe a multiplex test that has been developed to test and differentiate between flu and Covid infection from a single sample.
https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm
"Influenza (flu) and COVID-19 are both contagious respiratory illnesses, but they are caused by different viruses. COVID-19 is caused by infection with a coronavirus first identified in 2019, and flu is caused by infection with influenza viruses. [...]
Because some of the symptoms of flu, COVID-19, and other respiratory illnesses are similar, the difference between them cannot be made based on symptoms alone. Testing is needed to tell what the illness is and to confirm a diagnosis. People can be infected with both flu and the virus that causes COVID-19 at the same time and have symptoms of both influenza and COVID-19."
https://www.cdc.gov/coronavirus/2019-ncov/lab/multiplex.html
"The CDC Influenza SARS-CoV-2 (Flu SC2) Multiplex Assay is a real-time reverse-transcription polymerase chain reaction (RT-PCR) test that detects and differentiates RNA from SARS-CoV-2, influenza A virus, and influenza B virus in upper or lower respiratory specimens. The assay provides a sensitive, nucleic-acid-based diagnostic tool for evaluation of specimens from patients in the acute phase of infection."
-
2
-
1
-
1 hour ago, Freddy42OZ said:
Bangkok does not have to be expensive.
The building I live in is 100m from a BTS station that will get you to Asoke in under 20 minutes.
50 sq/m 1 bedroom condo will cost you 10-11,000 THB, a 50 sq/m 1 bedroom corner unit with balcony 14K, 70 sq/m 2 bed around 22K.
20 minutes to Asoke means the terminal end of the BTS, either Mo Chit or Bearing, or an equivalent distance. I consider that to exactly fit my description "way out" as you can't travel any further from the centre than that on BTS !
EDIT: Well I'm wrong here, as they have extended the BTS further than when I used to live in Bangkok, so you CAN live further out and still be on the BTS.
Nevertheless I still consider my assessment of these former terminal stations as being "way out" to be a fair description...(I lived at Asoke)
-
2
-
-
- Popular Post
Bangkok is expensive, and if you want to live a reasonable life the UK state pension (which I presume you mean, though don't say directly) is probably not enough alone, especially as there are no cost of living increases, so in 10 years it will have lost enormous value.
Decent accommodation , ie not a 35m2 room could cost 15-25,000B unless you live way out. You need health insurance, as a serious illness if uninsured can wipe out half your savings or more. If you eat western food it will triple food expenses.
As has been pointed out, it is getting more and more difficult to keep a UK bank account with a foreign address, so you need to take steps to open an offshore account which will not be in danger of sudden closure with little notice.
With the amount you have it is certainly possible, without too much problem, if you are willing to diminish capital savings.
-
3
-
2
-
- Popular Post
- Popular Post
7 hours ago, ArcticFox said:Peer-reviewed study of the efficacy of Ivermectin published in the American Journal of Therapeutics: July/August 2021 - Volume 28 - Issue 4
Ivermectin for Prevention and Treatment of COVID-19 Infection: A Systematic Review, Meta-analysis, and Trial Sequential Analysis to Inform Clinical Guidelines
https://journals.lww.com/americantherapeutics/Fulltext/2021/08000/Ivermectin_for_Prevention_and_Treatment_of.7.aspxThis meta analysis is untrustworthy and out of date as it actually contains, and is strongly skewed by, the faked data paper by Elgazzar et al, which has been withdrawn because the data was made up. Obviously this meta analysis will have to be re-done by the authors because it includes known and withdrawn false data, and its conclusions do not count. This is simply unarguable.
The Elgazzar paper showed so such a statistically strong positive effect for ivermectin (because it was faked) that its inclusion alone in meta-analyses can distort the results in favour of a positive effect where none exists- especially if the data, as in this meta analysis -is termed low or moderate certainty evidence.
Here is the statement by an epidemiologist reported in the Guardian UK on 16th July this year after the Elgazzar paper was revealed to be false.
"Meyerowitz-Katz told the Guardian that “this is one of the biggest ivermectin studies out there”, and it appeared to him the data was “just totally faked”. This was concerning because two meta-analyses of ivermectin for treating Covid-19 had included the Elgazzar study in the results. A meta-analysis is a statistical analysis that combines the results of multiple scientific studies to determine what the overall scientific literature has found about a treatment or intervention.
“Because the Elgazzar study is so large, and so massively positive – showing a 90% reduction in mortality – it hugely skews the evidence in favour of ivermectin,” Meyerowitz-Katz said.
“If you remove this one study from the scientific literature, suddenly there are very few positive randomised control trials of ivermectin for Covid-19. Indeed, if you get rid of just this research, most meta-analyses that have found positive results would have their conclusions entirely reversed.”
I find it really psychologically interesting that people choose to believe, with no evidence at all, and no basis in fact that "big pharma" are somehow suppressing ivermectin use, and yet when it is actually reported with evidence and withdrawal of studies that University research groups have literally been found to be making up data to falsely show ivermectin is effective, this is ignored!
-
1
-
3
-
8 hours ago, TigerandDog said:
that was a different statement. The one I'm referring to was saying the German report on the success of mixing single doses of AZ and Pfizer was incorrectly reported. The tests that the German report was referring to were actually for 2 doses of AZ then 2 doses of Pfizer. They also clarified in that report that testing was still ongoing in relation to mixing single doses of AZ & Pfizer. In fact WHO came out in a press release on 13 July ( one month after the German report and their subsequent statement saying that German report was incorrect ) and stated that single dose mixing and matching of different vaccines was not recommended until further testing had been completed.
I don't understand this at all - I think maybe you have misunderstood what you have read?
Firstly there are only two German studies that I can find that trial mixing doses of the Astra Zeneca (ChAdOx1) adenovirus vaccine and the Pfizer (BNT162b2) mRNA vaccine.
Both are published as preprint papers on the medrxiv server, and both clearly report in their methods section that they study the results of a single dose of each vaccine, and not two doses of each. I give you the links and actual extracts of the papers detailing their dosing methods below at the end of the post.
There is no way any WHO statement can override or correct the dosing methods stated in print by the actual researchers in their papers, so this seems a very unlikely statement for them to make.
Moreover I can find no trace of any WHO statement which actually does this with reference to doses. The one you link to on July 13th [https://www.reuters.com/business/healthcare-pharmaceuticals/who-warns-against-mixing-matching-covid-vaccines-2021-07-12/] does not mention doses at all. While they certainly recommend against mixing vaccines, they do not discount this altogether.
It says private individuals should not decide whether to mix vaccines, but state or public health agencies should make this decision. The actual Reuters article you link to specifically quotes the WHO saying:
"The WHO's Strategic Advisory Group of Experts on vaccines said in June the Pfizer Inc (PFE.N) vaccine could be used as a second dose after an initial dose of AstraZeneca (AZN.L), if the latter is not available."
I may have not been able to find the WHO statement you mention with dosing information-if so I apologise and would appreciate a link or quote.
***********
The German papers describing single dosing with each vaccine:
1. https://www.medrxiv.org/content/10.1101/2021.06.01.21258172v1.full-text
Humoral and cellular immune response against SARS-CoV-2 variants following heterologous and homologous ChAdOx1 nCoV-19/BNT162b2 vaccination Barros-Martins, J et al (2021) " Vaccinees who received one dose of ChAd were, according to the current vaccination strategy in Germany, offered to choose between ChAd and BNT vaccines for a second dose. "
2. https://www.medrxiv.org/content/10.1101/2021.05.19.21257334v2.full.pdf+html
Safety, reactogenicity, and immunogenicity of homologous and heterologous prime-boost immunisation with ChAdOx1-nCoV19 and BNT162b2: a prospective cohort study Hillus D, et al (2021) "Study participants either received two doses of BNT three weeks apart or an initial dose of ChAdOx followed by a heterologous boost with BNT 10-12 weeks later, in accordance with the recommendations of the German standing committee on vaccination (STIKO)."
-
2
-
-
- Popular Post
- Popular Post
Both alcohol and Ibuprofen (and related compounds - NSAIDS- non-steroid anti-inflammatory drugs) are suppressors of the immune system and therefore the immune response.
As the idea of vaccination is to trigger a strong immune response to the antigen in the vaccine, in principle you do not want to reduce its effectiveness by suppressing any part of the immune response.
Whether the effect of either of these substances on the actual immune response to a vaccine is significant or trivial isn't really clear though.
-
1
-
2
-
2 minutes ago, Strongheart said:
If you lack the knowledge to comprehend my comment then why don't you research STERILE IMMUNITY and Prophylactic Gene Therapy instead of twisting your panties into a bunch, comrade.
You are the one who lacks knowledge since the comment you are replying to is correct in every way whereas your original post is nonsense.
-
- Popular Post
- Popular Post
2 hours ago, fearless1 said:I take about 17 grams every one or two weeks (it's not an exact science and there are different prophylactic protocols). Generally, they all seem to involve taking approximately .2 mg/kg per dose which for me is about 3 and 1/2 pills.
I take 3000 to 5000 iu's of vitamin D per day and 30 mg of zinc per day. I take other supplements too but the vitamin D and Zinc are the most critical in terms of protection related to covid.
I generally drink a couple of glasses of wine per day and I have never noticed any problems with that. Keep in mind that over 4 billion doses of ivermectin have been administered over the last 30 years or so and the only side effects have generally been related more to the die-off of parasites than anything else. It's much safer than statins or ibuprofen.
Yes, but what all you guys who think social media is a better guide to health matters than science seem totally unaware of, is that the prophylactic treatment for parasites is one dose of ivermectin, every 3 months to a year!
None of the 4 billion doses are taken by people every day or every week!
Additionally you don't actually know whether you are having side effects or not. Just because you don't feel anything does not mean no harm is occurring, does it?
If it did, then everyone who has early cancer, high blood pressure, and many other diseases would be aware of it straight away, rather than realising it only when the damage done becomes serious enough to show symptoms.
See dosages here https://www.medicalnewstoday.com/articles/ivermectin-oral-tablet#dosage
Extract:
"Take as directed
Ivermectin oral tablet is used for short-term treatment. It comes with serious risks if you don’t take it as prescribed.
If you stop taking the drug suddenly or don’t take it at all: Your parasitic infection won’t be cured.
If you take too much: This is not likely because in many cases, you’ll take this drug one time only, as a single dose. However, if you take too much or your dose is too high, you could have dangerous levels of this drug in your body
Dosage for parasite infection in the intestinal tract
Adult dosage (ages 18–64 years)
Typical dosage: 200 mcg/kg of body weight taken as one dose. Most people won’t need more than one dose.
Dosage for parasite infection in skin or eyes
Adult dosage (ages 18–64 years)
Typical dosage: 150 mcg/kg of body weight taken as one dose.
Follow-up treatment: You’ll likely need follow-up care from your doctor and additional rounds of treatment with this drug. Your doctor will decide when you’ll receive your next dose of ivermectin. You may be treated again in as few as three months.
-
13
-
5
-
- Popular Post
- Popular Post
32 minutes ago, DoctorB said:Indeed; why should 2022 be any different? Vaccination?
Really? The top headline in the Daily Mail today is : "Freedom Day will cause a mad spike in covid cases and tens of thousands will die if Britain rushes back to normal life, leading scientists warn", yet the UK has vaccinated over 70% and up to 90% are thought to have covid antibodies. So "top experts" in the country that has been at the front of vaccinations have no faith in what has been achieved. The implication would seem to be that all government action is pointless except lockdowns and we can only be released when the virus has passed naturally.
Not correct. Only 54% have been fully vaccinated with the double dose tested in all clinical trials and on which effectiveness estimates are based. 69% have received at least one dose. These percentages refer to the entire population, including children.
The 90% figure you give for antibody positivity is for adults only, therefore excludes everyone under 16-18, which is between 20 and 25% of the population. Therefore at least 30% of the entire population have no protection at all, and around 15% only partial protection from a single vaccine dose.
30% of 60 million is 18 million potential infections, and 18 million potential factories for new variants.
The scientists do have faith in what's been achieved, but are warning that what has been achieved is incomplete, and that the lockdown restrictions have been lifted too completely, and too early in the vaccination roll-out.
They will be proved correct.
-
4
-
 1
1
-
- Popular Post
- Popular Post
Just as a heads up , for those unaware- the major paper with amazingly positive results for ivermectin that tips most meta-analyses towards positivity has been shown to be fabricated, and withdrawn "for ethical reasons".
The Elgazzar study from Benha University Egypt supposedly found that patients with Covid-19 treated with ivermectin showed “a substantial improvement and reduction in mortality rate in ivermectin treated groups” by 90%.
Among the discrepancies discovered in this paper:
1. Introduction copied from websites and press releases, but altered individual words using synonyms to try to avoid detection.
2. Contradictory claims within the paper itself, e.g. patients said to be aged 18-80 but 3 patients in data set were under 18; study claimed to be done between 8th June and 20th September 2020, but most of the patients who died were admitted and died before 8th June 2020; paper says there were 4 deaths in mild Covid patients treated with standard treatment compared to 0 deaths in ivermectin group - the raw data gives 0 deaths for both groups; paper says there were 2 deaths in severe Covid patients treated with ivermectin the raw data shows there were 4 deaths.
3. Fabricated data: about 79 of the patient records were obvious near-identical copies of other records, but clear evidence of fraud shown by deliberate minor changes in some of the details, so data simply repeated to try to falsely bump up number of patients in the trial.
This is reported in the Guardian July 16th
Here's an extract giving the opinion of Australian chronic disease epidemiologist from the University of Wollongong, Gideon Meyerowitz-Katz:
"Meyerowitz-Katz told the Guardian that “this is one of the biggest ivermectin studies out there”, and it appeared to him the data was “just totally faked”. This was concerning because two meta-analyses of ivermectin for treating Covid-19 had included the Elgazzar study in the results. A meta-analysis is a statistical analysis that combines the results of multiple scientific studies to determine what the overall scientific literature has found about a treatment or intervention.
“Because the Elgazzar study is so large, and so massively positive – showing a 90% reduction in mortality – it hugely skews the evidence in favour of ivermectin,” Meyerowitz-Katz said.
“If you remove this one study from the scientific literature, suddenly there are very few positive randomised control trials of ivermectin for Covid-19. Indeed, if you get rid of just this research, most meta-analyses that have found positive results would have their conclusions entirely reversed.”
The discover of the fraud, a med student (!) said
"Thousands of highly educated scientists, doctors, pharmacists, and at least four major medicines regulators missed a fraud so apparent that it might as well have come with a flashing neon sign. That this all happened amid an ongoing global health crisis of epic proportions is all the more terrifying."
-
2
-
1
-
18 hours ago, Puccini said:
It looks like the police has not yet gone after this example of fake news:
SteriPlant sanitising product kills COVID-19 in 1 minute (proven in lab tests)
There's no reason to assume this is fake news. Soap and water kills the Covid-19 virus in 20 seconds.
It's just completely useless as a drug as, with 99.9% certainty, this will also turn out to be.
-
- Popular Post
- Popular Post
23 hours ago, DeepSea said:I don't know if you took the time to actually look at any of this data, but let me give you an example.
If you open the linked document, then search for 'Ahmed (DB RCT)' (listed in the first chart, below the summary in Blue at the start of the document). Mouse over the name and click on the hyperlink, which will take you to this document. The header on this document is described as follows:
Ahmed et al., International Journal of Infectious Diseases, doi:10.1016/j.ijid.2020.11.191 (Peer Reviewed)
A five day course of ivermectin for the treatment of COVID-19 may reduce the duration of illnessIt cites the name of the publication, a reference number and a brief description of the study, some of which are pre-prints, others are peer reviewed. Below that is a hyperlink to the SOURCE, this is where you will find the names of those responsible for each study and in many cases the name of the medical institution they are affiliated with. From what I can see this source material is available for all of the studies provided, not exactly anonymous as you suggest... They may work as plumbers in their spare time, perhaps you can do a little more research and find out?
I was very obviously referring to the authors of the meta-analysis as being anonymous of course, not the authors of the papers which are used within the meta-analysis, and which are public domain. Let me emphasise: science is about open and free and attributable exchange of ideas. Authors of papers who do not want to reveal who they are are not trustworthy
The meta-analysis itself is a huge squid ink splurge of all the data, coupled with sensationalist and statistically invalid statements like
"As above, the probability that an ineffective treatment generated results as positive as the 62 studies to date is estimated to be 1 in 652 billion (p = 0.0000000000015)."
that no serious scientist would write.
-
2
-
1
-
On 7/4/2021 at 5:49 AM, DeepSea said:
I posted a link to a totally transparent, real-time meta analysis of 61 studies (which also includes a couple of negative results), which I'm sure you haven't read, would you care to reciprocate by linking us to your list of negative clinical trials?
If you think a non-peer reviewed, anonymous, that is the authors don't actually dare to reveal who they are, (are they plumbers, geographers, experts in data analysis ?) screed on a commercial .com site is "transparent", then you have a rather elastic definition of this term.
They do declare they are "Ph.D scientists, and you can find our work in journals like Science and Nature," but of course it's not really possible to check is it?
I am a Ph.D scientist and you can also find my work in Science and Nature, if you look hard enough.
-
2
-
-
26 minutes ago, Harry Om said:
"The median time to resolution of symptoms was 10 days (IQR, 9-13) in the ivermectin group compared with 12 days (IQR, 9-13) in the placebo group"
It didn't reach statistical significance, but you were still better off being in the Ivermectin group.
It's worth noting that the claim with Ivermectin is that it works best if used early as possible to reduce viral load. Once you're in hospital then it's too late, the damage is already done. So some of these studies are after the horse has already bolted, so it's not suprising their findings aren't conclusive.
You aren't better off in the ivermectin group. The P value is 0.53 which means that the chance of this being purely random statistical fluctuation indicating no difference between groups is 53%- that is the same as tossing a coin.
The acceptable P value for a difference to be accepted in a study like this is 0.05, that is there is a 1 in 20 chance of this difference being a chance occurence .
-
1
-
-
47 minutes ago, tifino said:
dumped all the Scripts for the 'Statins, and adopted CoQ10 over the counter... '
whereas 'Statins rip the guts out of both HDL and LDL (one likens Statins as the medicine cabinet equivalent of 'RoundUp in the garden' - where they are non selective in what they get rid of!!
Losing HDLs alongside the happy to be ridden of LDL - means the body then does not have enough HDL left inside, to do their ongoing battles on bad cholesterol.'
CoQ10 rids the LDLs, ut Not at the expense of the reserves of HDL that 'are' needed
Mostly wrong I'm afraid, being completely contrary to evidence gathered from numerous clinical trials.
The most incorrect statement you make is that statins reduce HDL. In fact statins raise HDL, they don't decrease it! Different statins do it to different degrees, but this has been seen with all.
See, for example, this paper -link- https://pubmed.ncbi.nlm.nih.gov/20513953/
Molecular mechanisms of HDL-cholesterol elevation by statins and its effects on HDL functions
Shizuya Yamashi ta 1, Kazumi Tsubakio-Yamamoto, Tohru Ohama, Yumiko Nakagawa-Toyama, Makoto Nishida
Journal of Atherosclerosis and Thrombosis 2010 May;17(5):436-51.
"Numerous large-scale clinical studies have revealed that the low-density lipoprotein cholesterol (LDL-C)-lowering effect of 3-hydroxy-3-methylglutaryl-CoA (HMG-CoA) reductase inhibitors (statins) prevents coronary heart disease (CHD). Statins have not only LDL-C-lowering effects but also high-density lipoprotein cholesterol (HDL-C)-elevating effects, which differ among statins."
Statins have been shown to reduce all cause mortality, in addition to mortality caused by coronary artery disease, which somewhat contradicts your unsubstantiated claim that statins don't allow the body to battle ' bad cholesterol'.
See, for example, this analysis of 18 separate randomised clinical trials of statins, where results of all the trials are combined and statistically re-analysed as a whole -link- https://pubmed.ncbi.nlm.nih.gov/23440795/
Statins for the primary prevention of cardiovascular disease
Fiona Taylor 1, Mark D Huffman, Ana Filipa Macedo, Theresa H M Moore, Margaret Burke, George Davey Smith, Kirsten Ward, Shah Ebrahim Cochrane Database Systematic Reviews 2013 Jan 31;2013(1):CD004816
"Main results: The latest search found four new trials and updated follow-up data on three trials included in the original review. Eighteen randomised control trials (19 trial arms; 56,934 participants) were included.[...]
All-cause mortality was reduced by statins (OR 0.86, 95% CI 0.79 to 0.94); as was combined fatal and non-fatal CVD [coronary vascular disease] RR 0.75 (95% CI 0.70 to 0.81), combined fatal and non-fatal CHD events RR 0.73 (95% CI 0.67 to 0.80) and combined fatal and non-fatal stroke (RR 0.78, 95% CI 0.68 to 0.89). [...] . There was no evidence of any serious harm caused by statin prescription."
Finally CoQ10 has not been shown to have any significant effect at all on LDL levels, though it does seem to raise HDL levels in trials, so this is the single correct statement in your post!- see link- https://pubmed.ncbi.nlm.nih.gov/30296936/
The effects of coenzyme Q10 supplementation on lipid profiles among patients with coronary artery disease: a systematic review and meta-analysis of randomized controlled trials
Mohammad Vahid Jorat 1, Reza Tabrizi 2, Naghmeh Mirhosseini 3, Kamran B Lankarani 4, Maryam Akbari 2, Seyed Taghi Heydari 4, Reza Mottaghi 5, Zatollah Asemi 6 Lipids in Health and Disease 2018 Oct 9;17(1):230
"Results: A total of eight trials (267 participants in the intervention group and 259 in placebo group) were included in the current meta-analysis. The findings showed that taking CoQ10 by patients with CAD significantly decreased total-cholesterol (SMD -1.07; 95% CI, - 1.94, - 0.21, P = 0.01) and increased HDL-cholesterol levels (SMD 1.30; 95% CI, 0.20, 2.41, P = 0.02). We found no significant effects of CoQ10 supplementation on LDL-cholesterol [...]"
-
1
-
-
You could try to phone them and ask. It's probably OK, as there are now very long delays in assigning received payments to individual accounts. If you call them they will be able to tell you if the payment has been received and can assign it to your account immediately after you call.
I'm not overseas any more, but made a class 3 voluntary payment in the UK on Jan 25th this year, and phoned them 5th March to check, as it had not shown up. They told me it had been received but was in the queue for being assigned, and that they would do it that day.
I appreciate it's expensive to call from abroad: they play a lot of prerecorded messages and I had about a 20 minute wait after that, but it may be worth it for your peace of mind.
The HMRC NI contributions help desk number I used in the UK was 03002003500, but I'm not sure if this works from abroad , so you may have to Google for information about whether you need to contact a different department concerning overseas NI contributions.
-
1 hour ago, CALSinCM said:
Same with the PCR test. Considering there are no globally accepted standards for PCR cycle counts, there is a (significant) risk of an inconclusive (false-positive) result.
The CDC recommends a cycle count of 28 for vaccinated people. But that's the problem. For vaccinated people. So they themselves openly promote using non-standard cycle counts: one CT for vaccinated, and another for unvaccinated.
That's manipulating the outcomes. Purposefully. It's unethical. And the fact is that labs world-wide to set the cycle count to anything. Which is unreliable.
The cycle-count should be set to 28 as a global standard for everyone.
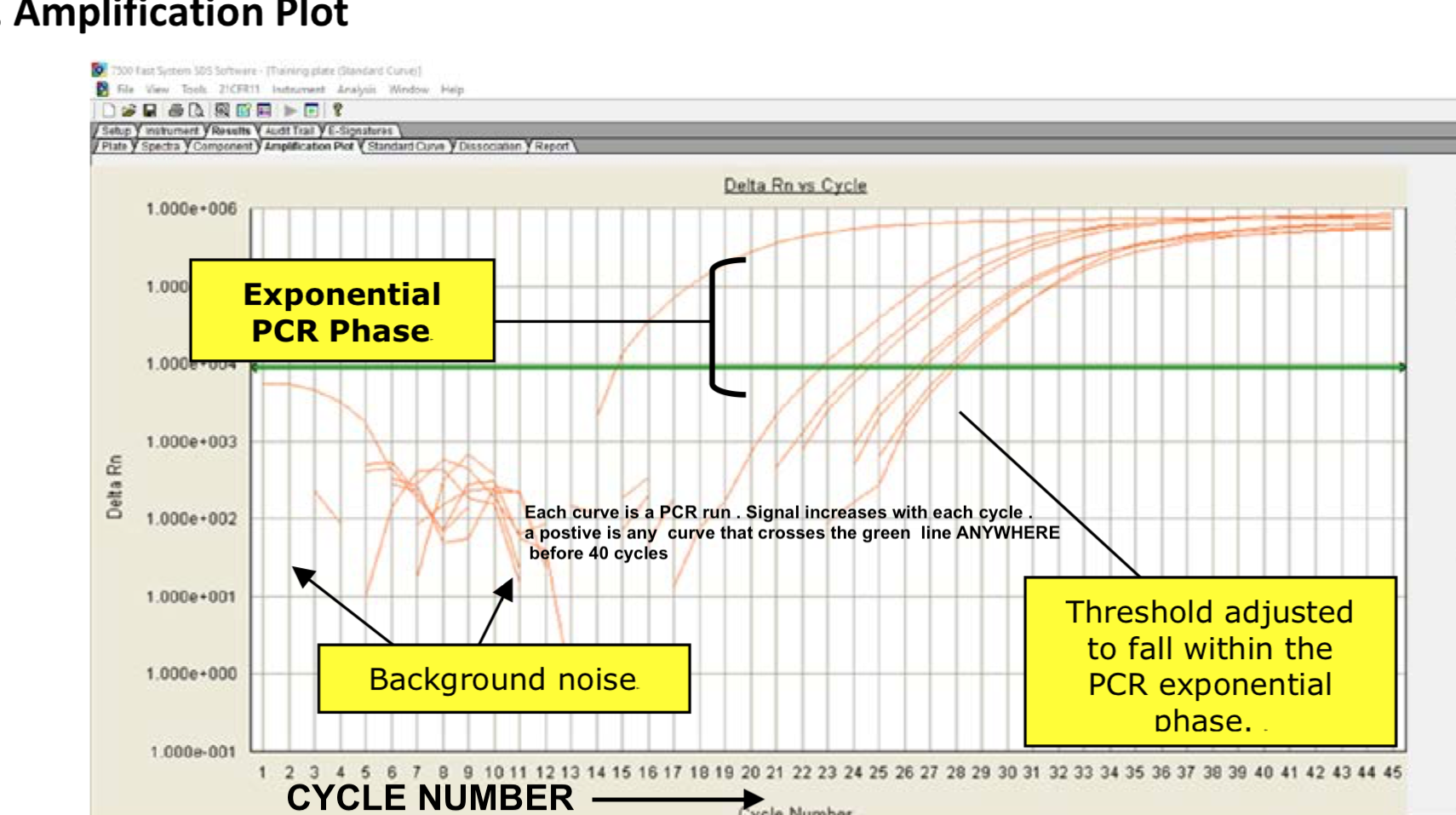
But without a standard cycle-count? There is too much risk to travel to Thailand imho.I would like a reference or citation for these claims that you make, as they seem a bit nonsensical at first glance.
Firstly the quantitative PCR method used to detect a positive or negative result is not based on a fixed number of cycles being defined.
Without going into too much detail: all samples are run for ~45 cycles, with a positive control standard (known RNA representing viral sequences) and a negative control (water). After the run curves are drawn and a horizontal threshold line is drawn across joining where all the curves start to become exponential [see fig. below]. A positive result is when any sample crosses this threshold before 40 cycles.
reference from cdc https://www.fda.gov/media/134922/download
This being the case I find it hard to see how the cdc could recommend a fixed number of cycles for any samples, from vaccinated people or not
If you can point to a reference or citation, [for example you might be referring to a completely different RT-PCR test that I'm unaware of] I will quite happily admit that I am mistaken.
-
- Popular Post
- Popular Post
6 hours ago, OJAS said:As @flexomike has stated, he is aware of several Thais who are collecting Social Security in Thailand and they are not US citizens. So why can't British nationals collect in the UK by the same token?
They can and do. It is completely legal and no US citizenship, residence, or current green card status is necessary.
Even a cursory glance at eligibility requirements on the US SSA site will show you this, but if you can't be bothered:
I am a British citizen. I worked in the US for 12 years on a green card, so accumulating more than the 40 social security contributions necessary to earn a social security retirement benefit. About 10 years ago I left the US, filling in a final tax form informing the IRS of my departure, and shortly after officially gave up my green card at a US Embassy. All relevant government departments were therefore aware of my departure and my lack of us citizenship.
Three years ago I applied for my US social security retirement benefit through the Federal Benefits Unit at the London US Embassy, giving the information that I now lived permanently in the UK, was not a citizen, and had no residence rights in the US as I had surrendered my green card.
They deposited the first benefit payment directly into my UK bank account and have done so monthly ever since.
-
2
-
4
-
7 hours ago, Stargrazer9889 said:
Straight whiskey is also okay but still lots of sugar.
No.
There is barely any measurable sugar in whisky at all.
https://www.verywellfit.com/scotch-whisky-nutrition-facts-and-health-tips-4844515
Scotch Whiskey Nutrition Facts
The following nutrition information is provided by the U.S. Department of Agriculture (USDA) for one shot (42g or 1.5 ounces) of scotch whiskey.1
- Calories: 97
- Fat: 0g
- Sodium: 0.42mg
- Carbohydrates: 0g
- Fiber: 0g
- Sugars: 0g
- Protein: 0g
- Alcohol: 14g
* This also applies to US bourbon whiskies as well, by the way:
-
2
-
7 hours ago, Cake Monster said:
Any Fruit combined with Alcohol will be a problem.
The Sugars that are omni-present in all Fruits will turn into Alcohol in the Gut while being digested.
Remember Fruit Punches ?
Biochemically this is nonsense. Humans do not possess enzymes that can turn sugar into alcohol, this is what yeasts do!
A medical condition does exist where some people have an abnormally high level of certain yeasts or abnormal bacteria in their small intestine, sometimes as a result of very prolonged treatment with certain antibiotics.
This condition is incredibly rare, so that in a study of the condition in the US, the authors considered themselves lucky to have been able to accumulate as many as 28 patients from the entire country (see https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6475837/).
This extreme rarity means the idea that fruit will be converted to alcohol in your gut applies to nearly no-one, and should not be taken seriously!
-
1
-
-
- Popular Post
- Popular Post
8 hours ago, doggie1955 said:Here is an update on Ivermectin... READ
This unfortunately is a non-peer reviewed paper commissioned by a commercial company hoping to sell a sustained release formulation of ivermectin to treat Covid-19, but who have done no clinical studies at all to prove that ivermectin is effective in treating Covid-19.
They simply report that giving the doses already shown to be safe for anti-parasitic activity at single dose daily for a month is also safe.
Their report directly states the steady plasma concentration of ivermectin achieved by this month long regime is 30ng/ml = 0.034µm.
The problem is that this is 60 times lower than the dose shown to be necessary in dishes of cells to have anti-viral effects against SARS-CoV-2 ( 1750ng/ml or 2µM), so it does not address the basic problem already referred to here
Antiviral Research June 2020 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7172803/
that the blood concentration achieved would not, on current understanding, be great enough have any significant anti-viral effect on SARS-CoV-2.
A correctly conducted and powered clinical trial proving that ivermectin is effective at treatment or prevention of Covid-19 is therefore crucially important.
-
3
What Worried You More?
in COVID-19 Coronavirus
Posted
There is no unwillingness to report these numbers, and it is simple common sense that when a vaccine is reported in the press to have efficacies of say, 85%, 70%, or 95% , it means that this is the percentage of people who are prevented from getting Covid after vaccination, compared to those who are unvaccinated.
Clearly this also directly informs you that 15%, 30% or 5% of people who are vaccinated will get Covid despite their vaccination status. There is nothing hidden or obscure about these statements!
Contrary to your implication that this is somehow hidden or deliberately obscured information, the mainstream UK newspaper The Guardian published a helpful article detailing exactly this only a month or so ago:
https://www.theguardian.com/theobserver/commentisfree/2021/jun/27/why-most-people-who-now-die-with-covid-have-been-vaccinated
"Why most people who now die with Covid in England have had a vaccination
David Spiegelhalter and Anthony Masters
It could sound worrying that the majority of people dying in England with the now-dominant Delta (B.1.617.2) variant have been vaccinated. Does this mean the vaccines are ineffective? Far from it, it’s what we would expect from an effective but imperfect vaccine, a risk profile that varies hugely by age and the way the vaccines have been rolled out.
Consider the hypothetical world where absolutely everyone had received a less than perfect vaccine. Although the death rate would be low, everyone who died would have been fully vaccinated.
The vaccines are not perfect. PHE estimates two-dose effectiveness against hospital admission with the Delta infections at around 94%. We can perhaps assume there is at least 95% protection against Covid-19 death, which means the lethal risk is reduced to less than a twentieth of its usual value."