


Mister Fixit
-
Joined
-
Last visited
Posts posted by Mister Fixit
-
-
- Popular Post
23 hours ago, Benmart said:I am grateful that I have resources to live here, but mostly that I have never met some of the creatures who post such hateful things about other people. It's the Russian government, not the individua Russian l tourist who is behind all this.
And it's the Russian people who 'voted' Putin in and they got what they wished for,
-
 3
3
-
 1
1
-
Many thanks for your technical contributions, chaps and when I've re-read them about 6 more times I will respond! ????
I have tried half a dozen times or more to get my free testosterone checked in Thailand and have been told the same number of times that they don't test for it here, only total testosterone. I read something above about calculating it from total test, but I speed-read both posts and only got the gist.
The thing is, I am due to see the andropause doc again on Tuesday next week, the 31st, so I would like to get some ducks in a row beforehand.
What's a 'must test for' that I haven't already had? (It's probably been mentioned in one of your posts, but could we make a list of what else to check?
The other interesting thing is the mention of bone density because I was told about 11 or 12 years ago that I have osteopenia, and take 1500 mgs calcium and Vit D twice daily.
I had a back X-ray the other week and that has deteriorated since the last one 3 years ago, but that's mainly cartilage thinning - but even I immediately noticed my spine was now not straight and has started to curve to the right slightly. I did have the L5 vertebra slightly misplaced 3 years ago but that has now expended to the L4 and the L2 and L3 are going too.
I don't have a lot of back pain though. A twinge here and there, but then again I've lost a total of about 55 kgs in the last 4 years which must have helped, at least somewhat.Let me digest all the stuff you've sent and thanks again for your help.
-
On 8/20/2021 at 9:02 AM, rott said:
I would imagine that instead of devoting 90% of his spare time to doing good works amongst the deserving poor he will increase that to 100%.
I would make so bold as to suggest that he assists me in a few projects such as giving cello lessons to the disadvantaged and to long term prisoners. Also teaching expats that there is no apostrophe in a plural and that could of and should of should be could have and should have.
When one door closes in life, another opens.
Time for my pill.
I just carry on doing my bits of part time teaching English and hence assist Thais in bettering their life.
If I could play the cello, maybe I would help you with that too.-
1
-
-
2 hours ago, worgeordie said:
What are you going to do , when all of these things
no longer work ,it will happen.will you be able to accept it.
regards Worgeordie
Nowt really te dee wi' ye, is it, wor kid?
It's been gannin' alang for a geet few months noo, marra, 'n' Aa've pretty well accepted what's gannin' on by noo.
Just is lang as Aa kin get a bit uh legower once a week, Aa'm happy. Ye canna change gettin' owld, but ye kin at least try t' slow things doon.
-
 1
1
-
-
Just now, rott said:
I do beg your pardon it was the Sidegra that caught my attention, they are the ones that came from a hospital pharmacy.
No problem. ????
Yes, Sidegra are 250 baht at the Nana pharmacy I use, but at the hospital they were only something like 152 baht. They worked well too! ????
-
1
-
-
On 8/16/2021 at 5:03 AM, MarkyM3 said:
Hi Misterfixit....
I have been on TRT in the UK for the last 3 years so have some experience of the highs and lows of it. I am currently using Nebido (have also done gels, which are a PITA ultimately and gave me skin problems). Fortunately, it's laid on free via the UK NHS (public health service) though I pay plenty of taxes so quid pro quo!
Some of the indicators your endo should be monitoring are not on that list. For example, to calculate free testosterone (i.e. available to bind to androgen receptors), it's done using raw testosterone plus SHBG and Albumin figures iirc. Can't see either of the latter 2 on there.
E2 (oestrogen), PSA (possible indicator of prostrate issues ahead) and haematocrit ratio (blood thickness), are important and can see those there. If E2 gets too high, Anastrozole can be introduced to lower it (but can cause problems). Prolactin should be on there but isn't.
Your figures are all in imperial measurements so I'd need to translate to the reference ranges I see when I do my bloods.
Also - not sure of your age and this may not matter but be prepared to see your balls shrink and ejaculate reduce. This apparently can be counteracted by HGC but isn't offered in the UK NHS. Am thinking of using a private doctor to get this looked at because I'm 50, unmarried and still might want to have kids in the next couple of years.
Shoot me a PM if you like and I can fish out my previous results to see if there's anything else to mention.
Sorry for the delay in replying to your post and PM. There's been too much going on.
Not too sure about them being Imperial measurements, which are UK. Thai hospitals tend to use US measurements. But I'm not familiar enough yet with all of them to be 100% sure of what's what.
I don't have a range for the E2 so I don't know if what is in that report above is high, low or average. It just says 46.90 pg/mL (which suggests a metric measurement). Do you know what the range should be? I have read conflicting reports.
How did you find the Nebido injections? I have heard they take up to 4 minutes to do! ????
And I'm 72. I'll reply to your PM later. Maybe better to keep it that way because I've asked about this quite a lot over the last few months and I'm probably boring people by now! ????
-
2 hours ago, rott said:
Which hospital pharmacy sells these magical Cialis as described in the OP.?
I didn't buy the Cialis from there, I got them from a small pharmacy near Nana. I said that in the OP.
But Phramongkutklao, the Army hospital near Victory Monument have them but they cost 472 baht each and as you can buy them at pharmacies around Nana for 2,000 baht for a strip of 4, so just go there. Much easier.
I doubt you'd get in to the Army hospital. I was wangled in by an old girlfriend, an Army nurse there about 11 years ago. Then a few years later, an old student who happened to be a nurse there heard my ancient knees cracking and got her husband, also a doctor there, to refer me to the orthopaedics department. I am very happy with my treatment there in all the departments I have been to.
-
-
On 8/14/2021 at 3:42 PM, spidermike007 said:
Walked away from the big pharma poison pills years ago. Since then used either Bali Mojo, or Gracku. The latter is amazing. Please do not start with the FDA warnings. They are total nonsense. The FDA is one of the most corrupt organizations in the world, and one of their sole purposes is to support the drug companies and deny the benefits of anything natural. They are basically a drug company mafia, as we have seen with the Covid vaccines.
Tried this once, complete rubbish for me. All it did was give me indigestion which put me off sex.
Also I would say it didn't give me a full erection, maybe a 75% to 80%-er and it didn't last long.
-
@WaveHunter @rcuthbert @jackdd
Just wondered if you guys have any comments on my figures above, seeing how you helped out so much in the past?
-
-
On 8/11/2021 at 2:01 PM, KannikaP said:
Anyone with knowledge of nutrition will know that a BALANCED diet consisting of fruit, nuts, meat, fish, pie & chips, water, barley, yeast & hops are necessary for good health.
Unless you want to lose weight, in which case only a reduction in intake will work.
Anyway, I have lost 55 kilos overall and maintained the loss after starting strict keto 4 years ago. Best thing I ever did. You can stick your balanced diets because if I eat almost any fruit or vegetable, my weight zooms up - I have a high sensitivity to carbs from those and proved it time after time.
-
On 8/8/2021 at 10:18 PM, Sheryl said:
Elevated LDH can be due to diet/lifestyle or genetic. Hers is high enough to warrant attention. Avoiding processed carbs (or at least minimizing them - note that this includes white rice) and more exercise might do the trick if she is willing.
The FSH result does nto suggest menopause but a single FSH reading is not too reliable at her age.
Very slight MPV elevation with a normal platlet count is of no significance
LH, estradial etc, cannot tell anything when unknown where she was in her cycle. Anyhow I question the need for those tests (and in fact most of what was done). As it is now clear she is not menopausal there is no reason for her to attend an andropause clinic.
I think with your wife the issue is: is this PMDD (which as nothing to do with "period pain" AKA menstrual cramps) or is it generalized anxiety/depression? And that answer can only be determined by charting her moods relative to her cycle over time. If it is PMDD, natural progesterone may help. As I said before, the hallmark of PMDD s tat the mood issues occur in the 2 weeks prior to menstruation and improve dramatically when the period arrives.
Do not expect an andropause clinic to know anything about PMDD.
Yes, I think you are right in your penultimate paragraph. I initially took my wife because the doc had suggested it, so that she could discuss MY ED problems with the doc and her perception of how things were, and perhaps by speaking in Thai together she could tell him better what had been going on. Also, to speak to him about the problems she had been having with her periods, whether or not she has started the menopausal process.
Instead, she seems to have discussed her, what do seem to me the anxiety/depression problems that you hit on, with him and that's why she ended up with venlafaxine. I had no idea of any of this - she had never said a word, although I could see she was moody and quiet at times. Whenever I asked her why, she just fobbed me off. Last week she told me she didn't want to worry me with her problems due to the 'greng jai' concept (which I disagree with). How can I help if I am not told what's going on? And like a typical middle-aged traditional Thai woman, she was reluctant to voice her feelings anyway.
She now tells me that since taking the meds, all the pain and tension in her neck, shoulders and upper back has gone and she no longer has whirling thoughts in a whizzing brain, so that's all good. I am happy for her to continue, now that I know what was going on.
She takes them about 6 pm and is usually asleep between 9 and 10 pm as they make her drowsy. It's hard to say how she is during the day at the moment as she can't open her traditional Thai massage shop so just mooches about cooking or watching TV. I work part time and tend to sit at my computer in another room for the rest of the time.
Generally though, after a bit of zombie-like behaviour for the first week, she seems to have settled down with the meds.
We just need to be sure that the meds are managed well and when she decides to come off, that the withdrawal is well managed.
As to the lipids, yes, I know that eating a lot of white rice is a problem for many Thais, and why so many have high cholesterol and are often diabetic, as well as adding all that unnecessary sugar to their food. She tends to mix white rice and that 'rice berry' black rice but not always. She never adds sugar to food, but she does eat a few sugary things, mainly fruit, rarely chocolate or biscuits.
About 3 months ago, before we went to the hospital, she started exercising for about 30 minutes every evening, mainly hula-hoop and stretching and bending exercises using the hula-hoop as a prop.
We're due another appointment at the end of the month so I think it's best to leave things to develop and see what the doc has to say then.
-
I have written about this in a number of previous threads but I wanted to update people with how things have been going at the Andropause clinic I have been attending.
Readers of previous threads will know I had been having testosterone shots every 3 weeks since 2015 and after a visit to the endocrine clinic, they referred me to the andropause clinic. At the same time, I started fortnightly shots of 250 grams of testosterone enanthate – here are the dates so far.
7 May Saw endocrine doc, started fortnightly shots
20 May 13 days
4 June 15 days
17 June 13 days
1 July 14 days
16 July 15 days
29 July 13 days
Next shot should be 12 August.
I have noticed quite a difference in 3 months – my beard is much stronger (I could get away with not shaving daily, but not now), my pubic hair has grown thicker (but I trim it short it for hygiene reasons - in the past I have been prone to bouts of tinea cruris - jock or dhobi itch), my short term memory is somewhat better and I have managed to have sex successfully at least once a week (although still using an ED med).
So we have managed. Sex can be temperamental – I still find that erections can fade away and return, sometimes 3 or even 4 times, but we always end up with an orgasm one way or another. Twice we have had a real good old ding dong session without any fading away. When it does fade away and we can’t be bothered to keep trying, we have developed a technique where we can still satisfy each other.
I first went there on 15th June after I had started on the fortnightly testosterone shots. The very nice doc there said too high a dose could affect haematocrit so he ordered blood tests. I went back 2 weeks later on the 29th and haemoglobin and haematocrit were both fine, a touch low perhaps.
Then he bought in a colleague and they had a long confab, resulting in them suggesting that I try Nebido at 6,300 baht a pop every 3 months! AND there will need to be a series of shots while they titrate the dosage.
At the time, I still had about 12 or more testosterone enanthate ampoules at home, so we left it that I would use those up first and then talk again. I have 7 left so at one every 2 weeks will take 14 weeks so we still have 3½ months to get organised.
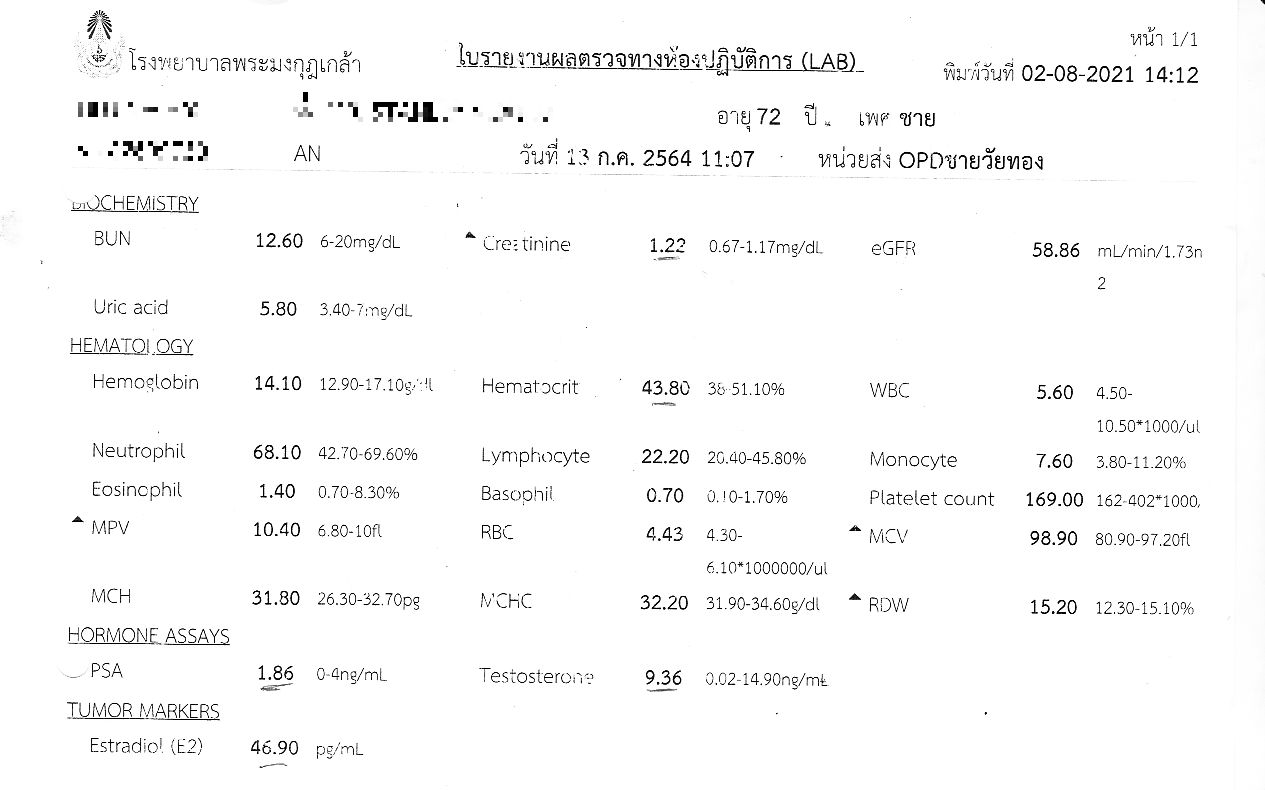
Then we returned 2 weeks later and he finally tested my oestradiol after I’d asked him previously. Having this tested had been mentioned by a few people in previous threads. I attach a copy of the report. I am pleased to see that my PSA still remains well below 4. My testosterone was OK at 9.36 with an upper limit of 14.90 ng/mL. That seems fine to me and he thought so too.
In terms of the oestradiol, it says 46.90 pg/mL, but there is no range mentioned. I have Googled and had conflicting results – Healthline says 10-40 pg/ml so mine is somewhat high.
Then I read a study abstract here https://pubmed.ncbi.nlm.nih.gov/7614406/ which said 10-82 pg/ml was normal – quite a difference!
Then I read on a website that levels were ‘Normal total estradiol levels in men are somewhere between 20–55 pg/mL (2.0–5.5 ng/dL) and 10-40 pg/mL (1.0-4.0 ng/dL), depending on whom you ask.’ https://tctmed.com/estrogen-in-men/
So, which is it? Does my figure look normal or too high?
Another thing I have learnt. I am now starting to believe that the pharmacy where I get my ED meds are selling, not necessarily fakes, but not true potency.
I used to use Sidegra but found it wasn’t as potent as Kamagra which I had always used before. I stopped the Sidegra and moved back on to Kamagra but found I was having to increase the dose to 1.5 tablets (or a 100 ml gel and half a 100 mg tablet which seems to work better) to get anything like a decent lasting erection, but even they were patchy.
I even bought a pack of supposedly ‘genuine’ Cialis from there, but the first one I took wasn’t much good, but the second was amazing. Really worked well and no problems. So I wonder if there are QC issues with what they sell or something.
Even more interesting was the doc suggesting I try Sidegra. I told him it had stopped being as effective and I’d stopped 18-24 months ago, but he suggested I tried again and got it from the hospital pharmacy so it will be authentic. I did and that night – wow! We were at it for getting on an hour and not a hint of a droop until about 45-50 minutes in.
Any comments on attached test results?
-
Late to the party, but Strattera (atomoxetine) IS available in Thailand.
It costs an arm and a leg though. I asked for some at Sritanya, the Government mental health hospital in Nonthaburi at the Ministry of Public Health. It was about 4,500 baht for a month's supply so I decided not to because it can take up to a month for results to be seen.
If it didn't work for me, what a waste of money - I can get 4 months worth of Ritalin for about the same amount.
However, if it works for you and the amount is OK for you, then try Sritanya (there's an MRT stop there on the Purple Line) and take a Thai with you because although the doctors all speak some English, most of the staff at registration etc don't.
-
On 7/16/2021 at 10:34 AM, The Hammer2021 said:
I consider Cialis superior. Try harder at a wider range of Pharmacies. I was warned of Zanax being in short supply soon too...possibly for the same reason. Another alternative is go for a check up at hospital get registered for ED or enlarged prostrate and get official prescription medicine
That's what I have done.
-
On 7/20/2021 at 10:28 PM, Sheryl said:
BOTH estrogen and progesterone need to be replaced. Indeed, replacing estrogen alone puts a woman at risk of uterine cancer. But that is nto the only reason, progesterone itself is very important. It is not produced only in pregancy (though levels in pregnancy are much higher). It is produced continuously and plays a very important role, especially in terms of mood stabilization. Indeed, while estrogen is what helps the hot flashes of menopause, progesterone is what often best helps the mood swings. Levels normally rise mid cycle and keep rising until menstruation, then drop.
Dermal creams and gels work very well for female HRT. Oral is not advisable as passes through the liver.
HOWEVER I note an earlier post from you states : "My wife started her menopause about 3 to 4 years ago and still has periods aged 52. ". This makes no sense. Menopause is defined as the cessation of menstruation. If your wife still menstruates, she is not yet menopausal.
Rather she is in the period known as "peri-menopause" and may nto need estrogen at all, though a blood test (FSH) will shed light on that.
During the peri-menopause many women develop PMDD (previously known as PMS) or, if they already had it, it worsens. It is very important to get the distinction between PMDD and menopause clear as the treatments differ and, in fact, estrogen would make PMDD much, much worse. PMDD responds to natural progesterone and, in severe cases, soemtimes needs the addition of low dose sertraline.
the hallmark of PMDD is that the symptoms occur somnewhere in the 2 weeks prior to menstruation (may start mid-cycle and last a full 2 weeks, or may start a little later in the cycle, but also continuing to menstruation) and then there is dramatic improvement when the period arrives - it feels like a curtain has suddenly lifted. Have your wife keep a diary of the timing of her symptoms. If they resolve once her period starts and she then has at least 10-14 days symptom free before it tarts again, this is PMDD.
Thai doctors are not well informed about PMDD.
Thank you for your long reply and improving my medical knowledge and vocabulary. PMS was just starting to be used as a term instead of ‘period pains’ when I first married in the 70’s and now it’s changed again! I had to Google the term PMDD because you didn’t explain it, but I get the idea.
I delayed replying because I wanted to see how we got on at the andropause clinic at our joint appointment last Tuesday so please allow me to report on events.
First, my wife – she chatted to the doc at some length, then I stuck my oar in to see what was being said or she’d not have told me.
Basically, the doc told me that she feels a lot better on the venlafaxine but is sleepier. Her anxiety and constant worrying over numerous small things (which she had never mentioned to me before in 14 years) has abated considerably and the pain and tension in her neck, shoulders and back has all but gone. I said I was disquieted by the use of venlafaxine because of considerable negative experiences I had had, especially coming off it, 18-20 years ago. I asked if she could go on something more innocuous, eg. fluoxetine or something similar but he said, and I understand this, that he wanted her to try at least one more month, possibly two, because it can take 4 – 6 weeks for the effects to kick in properly.
Fair enough by me but at the end of that period, I will want to be discussing continuance of the medication or changing it and the management of her cessation period. That can take a while. She may prefer to stay on it, and that’s her choice as long as when she decides to stop, it’s well managed.
Then we spoke about Oestrogel and he’s all for it but said she isn’t ready for it as she is still having periods regularly. Again, fair enough.
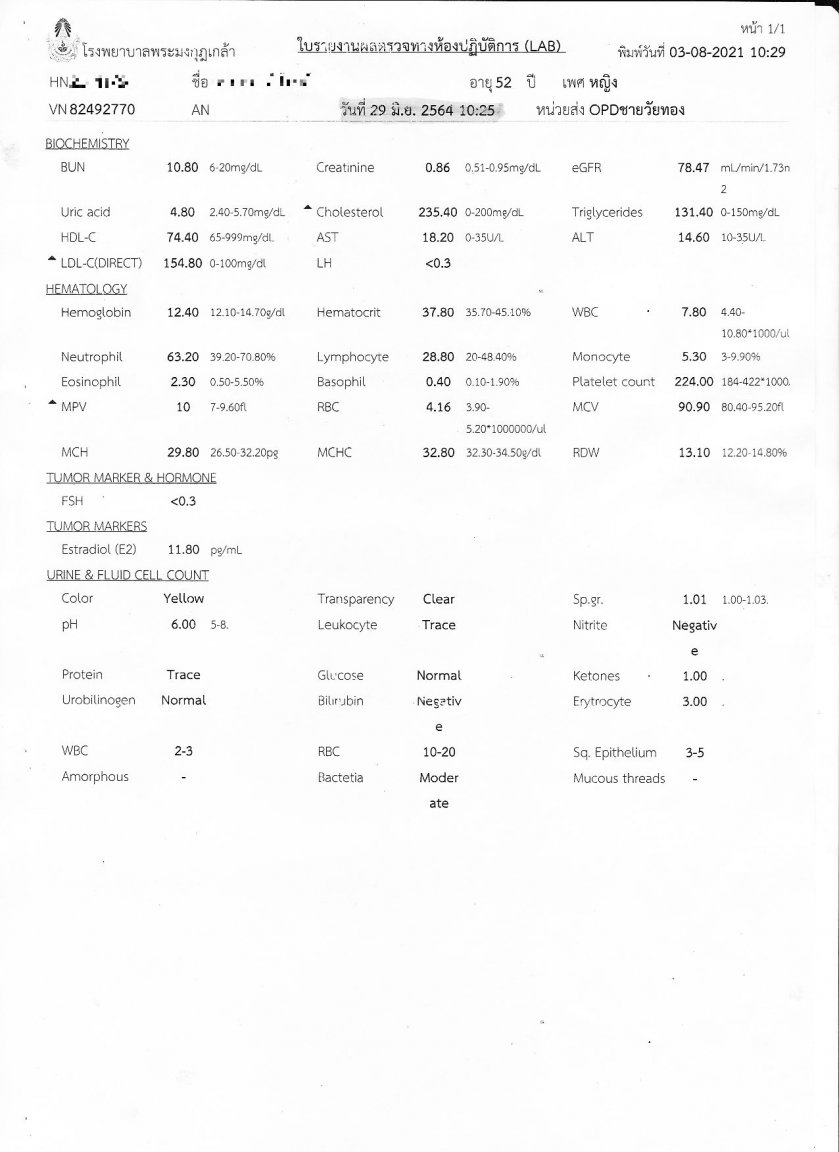
I asked for a copy of her 29 June test results (attached below) which were printed as we left so we couldn’t discuss anything at the time. I will next month though!
I attach a copy because although I understand some of the items, I am lost on others. I wonder if you could help with answering some questions?
In terms of the biochemistry, all looks OK apart from somewhat elevated cholesterol level at 235.4 (it would be 5.88 in the UK, where 5 is the number to aim for) so not massive.
Triglycerides are in the normal range so that’s OK. The HDL is a little low but within range. However, the LDL is way high – what can cause that and how can it be lowered?
LH (which I assume is luteinising hormone) just says <0.3 but I understand it depends on the phase of her menstrual cycle and I have no idea what that would have been at the time. Google tells me is seems low whatever phase she is in. Is this figure significant?
Her haematology figures all look within range except her MPV which I had to Google, but it’s not way above the top of the range. Any thoughts?
FSH just shows <0.3 with no range, but Google says for 41 years plus females ‘Any day of the menstrual cycle’ is = 0.5 ng/mL. Day 3 of the cycle for that age group would be < 8.5 mIU/mL.
Is there any significance to her figure in this report?
The figure for oestradiol (E2) doesn’t have a range, but Mr Google tells me that its 30 to 400 pg/mL for premenopausal women and 0 to 30 pg/mL for postmenopausal women so as my wife still has periods this figure seems low. Any ideas why this could be?
Urine test seems OK unless you can see anything in there that I don’t know about.
Most of this means nothing to me now, but I used to be very familiar with some of it 45 years ago when my first wife and I were having problems having children.
I will post again with my version of my own appointment and test results.
-
15 hours ago, Sheryl said:
Thai doctors tend to use synthetic hormones by mouth which is nto the best approach but all that most of them know
The best approach is bioidentical hormones via creams or gels. There is a bioidentical estrogen gel readily available OTC in Thailand (oestrogel) but sourcing bioidentical progesterone is problematic unless you order ti from iherb.
the various antiaging clinics ioffer bioidentical HRT and supposedly so does http://www.maximumclinic.com/womens-hormone-replacement-therapy/
You might point out to your wife than vebnlafaxine is hardly "natural" whereas bioidenticial HRT is.
I wouldn't DARE 'point out' anything to my wife! <grin - smileys still don't seem to work!>
Seriously, that's an interesting post and thanks for the tip on oestrogel. I will ask the doc about it in our next visit on 3rd August.In female HRT, do both hormones need replacing? I thought progesterone was only produced in pregnancy, but I am a bit out of date because my last child is now 26!
In terms of hormone gels, my utterly useless British GP prescribed Androgel for me but it did nothing.
As soon as I was properly diagnosed at Bumrungrad with hypogonadism due to pituitary adenoma and given testosterone enanthate every 3 weeks, things became much better. I lost weight, my memory improved, my general health also improved, my whole sense of well-being and, of course, my libido!
I believe that it has really helped my weight too. In 2004 I was 107 kgs, and now I am 71 kgs (but that was after 2 years of keto starting 2017, and 2 more years maintaining that weight.
I have actually lost 50 kgs or about 110 lbs overall, because 3 month long trips to the UK piled it all back on <about 6-8 kgs a time> and that had to be lost again).
-
16 hours ago, NancyL said:
I had to look that one up. Hmm. Couldn't that just be nature's way of telling you it's not a good idea to father children when you're getting up there in years?
And isn't menopause exactly the same when telling women not to bear children after 'getting up there in years'?
It's an unstoppable natural process but andropause normally comes much later in life for men. In my case, it was 'caused' (if that's the correct word) by me developing a cyst in my pituitary gland (a pituitary adenoma) when I was in my mid-50s and reduced my ability to produce testosterone naturally. I have to have regular injections to keep the levels up.
It's important for normal functioning - testosterone is not just a 'sex hormone'. It regulates mood, memory, bone and muscle mass, fat distribution and storage, production of red blood cells, semen, and of course, libido.
-
On 7/17/2021 at 4:47 PM, IvorBiggun2 said:
Absolutely. I was on and off antidepressants for 20 years. Been on a few over those years. Last one was Sertraline. In all those years I took the medication because I wanted it to work but in reality it hasn't/didn't. Looking back I see them as placebos and not worth the hassle. I stopped taking Sertraline 5th April and I'm determined never to go back on them.
What I do now when I get kind of depressed is to sit down and talk to the wife on how I'm feeling. I find talking about my moods to be far better than taking medication. Seems to be working so far.
Interesting to hear. In 1992, 30 years ago next January I discovered I had ADHD, but my useless British GP knew nothing about it and refused to refer me anywhere. I took matters into my own hands and I went to the US with my eldest son and we were diagnosed at the Massachusetts clinic of the world expert, Prof Russell Barkley. I got a supply of Ritalin in the States, but sadly, I was one of the 30% who don't respond to it.
Came back to the UK, took the report in to the doc and he still refused to believe it because 'it was American' (!) or to prescribe Ritalin. I knew Prof Eric Taylor of the Institute of Psychiatry in London so he wrote another report which convinced the GP, but still no Ritalin as he said I might sell it on the streets because I was unemployed at the time! Berk.
I ended up with so many different tricyclics, SSRIs and SNRIs note of which did me any good at all. I has so many different ones that I have forgotten the names of most of them.
Certainly, the two worst to come off were venlafaxine and sertraline, I do remember that. None of them were especially effective so I stopped the lot eventually, no need to keep banging your head against a brick wall.
Then I came to Thailand and threw myself into teaching and found I had a flair for it. I became extremely organised and was juggling sometimes 4 or more different classes a day (not every day) all over Bangkok between 8 am and 8 pm most days, so I had no choice but to be on time, find new places I hadn't been to and keep track of where students were in their book etc.
Hard work was the best thing to keep me on track. Still is.
-
On 7/18/2021 at 8:45 AM, NancyL said:
When I went into menopause my general doctor, an internist, recommended trying to wait out the undesirable side effects for six months before prescribing HRT because once you start on HRT, it can be difficult to stop.
Fortunately, my major side effect was hot flashes and since it was winter in Michigan and we kept our house cold, heating just the main living area with a wood stove, all I had to do was go into a colder part of the house or step outside during a hot flash. Eventually, everything settled out and I no longer had problems.
This was after decades of menstrual cramps, monthly moodiness, endometriosis, infertility, miscarriages. Finally peace. I overheard my husband telling a male friend at a party "menopause was much easier than I thought it would be." As if he was the one going through it!
I agree with my doctor on the subject of HRT. Don't rush into it. Give yourself six months or so to see if your body is going to settle down on its own first.
Nice helpful post. My wife started her menopause about 3 to 4 years ago and still has periods aged 52.
I think that's long enough to start considering a short course of HRT and be monitored regularly.
I have never experienced any female partners undergoing the menopause before so I am somewhat at a loss about modern HRT.
I have known women say it was a Godsend, but that was many years ago and medicine has moved on. The big thing then was injectable pellets but I have no idea at all how it is treated nowadays. Daily tablets, weekly/monthly injections?
What are the usual methods of treating it nowadays?
-
On 7/17/2021 at 11:24 PM, Sheryl said:
Well if she won't go on HRT then psychotropic meds may be necessary. As shame as the right HRT will often resolve these problems.
(Why bother going to a menopause clinic in this case?)
Why bother going? Because she asked to go when I started the andropause clinic. She has started the venlafaxine, but has only taken 3 tablets so far, so no time at all to see how or if they will help. She did say she felt a bit dizzy when she took them (she forgot yesterday) but I suspect that's just because she's new to them. I think that effect will wear off after a week or 10 days. We see the doc again on 3 August so I will be having a chat with him about the venlafaxine too. To my mind, it's a bit of a cosh and I remember having real problems myself when coming off it about 20 years ago. It took a few months, but I had a rubbish GP in the UK.
I know about VF being an anti-anxiety med and with the help of Google Translate, she agreed that that's what she experiences as well as being generally 'down' and worrying about many disparate things some time after her menopause started. That's been going a good 3-4 years now and still she has periods at 52.
She's a very traditional and old-fashioned middle-aged Thais woman and prefers Thai alternative medicine, which she studied for 6 years. She goes off to the department at the MOPH every so often for whatever it is she gets for her menopause symptoms. I am not much of a believer in alternative stuff, but it's ingrained in many older Thais.
And I have been talking about HRT with her quite a lot recently and I have suggested she tries a short course of whatever the doc suggests for 3 months and see how she goes.
I am sure she'll come round eventually because she has seen how good TRT has been for me. That's what piqued her interest initially, when I went to a different hospital and she saw how sympathetic and pleasant the doctors are there.
-
-
On 7/15/2021 at 10:04 PM, Sheryl said:
There is no point in asking people's experiences as everyone's reason for being on this medication will be different and few if any readers here will have been on it for menopause related issues. In addition, people vary enormously in how they respond to this medication.
The main advantage to venlafaxine is that, unlike many other antidepressents, it has an anti-anxiety effect as well. Whether or not your wife needs to be on an antidepressent/anti-anxiety med is another matter and obviously I have no way of knowing.
I do know that Thai doctors are not very up to date in management of menopause and that few places understand and use bioidentical HRT and the tendanecy here is to use synthetics. Synthetic HRT can sometimes cause depression, anxiety and other mental problems -- especially synthetic progestins. What has she been given in terms of hormones?
Nothing yet. Nor does she want to take any, more fool her IMHO.



Number of Russian visitors in Phuket instantly drops, Phuket struggles to find solutions for hundreds of stranded tourists with no access to funds due to sanctions
in Phuket News
Spot on, and not always under duress either.