partington
-
Posts
2,195 -
Joined
-
Last visited
Content Type
Events
Forums
Downloads
Quizzes
Gallery
Blogs
Everything posted by partington
-
 Resorting to false clickbait stories looks like desperation.
Resorting to false clickbait stories looks like desperation. -
Are we living in the Matrix?
partington replied to Phnom Penh Trader's topic in ASEAN NOW Community Pub
How they get ill-informed people to believe rubbish - like the recent Netflix series on the pyramids: 1. Find a plausible looking, but nutty, pseudo-academic who makes incorrect or simply made-up claims for which there is no factual evidence. 2. Show the majority of experts and researchers in the field explaining his claims are nonsense and unsupported by evidence. 3. To close the circle, claim triumphantly that experts in the field saying the claims are nonsense PROVES the claims are correct (because the experts are trying to cover them up). This will get large numbers of foolish people to follow this circular loop round and around forever, accepting more and more ludicrous nonsense. P.S. Here's the UK Guardian's much much more convincing theory about how such nonsense gets on Netflix in the first place (the program is "hosted" by a Graham Hancock): " how Netflix gave the greenlight to Ancient Apocalypse: the platform’s senior manager of unscripted originals happens to be Hancock’s son. Honestly, what are the chances?" https://www.theguardian.com/tv-and-radio/2022/nov/23/ancient-apocalypse-is-the-most-dangerous-show-on-netflix -
I should have truncated the quote from you to make it clearer so I apologise for that. I agree of course that human milk is better for early infants than cow's milk or formulas, until weaning. My objection was to this assertion, not the rest: which is not supported by nutritionists. For example, see below from McGill University. No suggestion here at all that adults or children shouldn't be drinking cows' milk, in fact it is recommended as a valuable nutrient resource. Consumption of Milk and Alternatives and Their Contribution to Nutrient Intakes among Canadian Adults: Evidence from the 2015 Canadian Community Health Survey-Nutrition. Auclair et al Nutrients (2019) Aug 19;11(8):1948. Abstract As a staple food and dense source of nutrients, milk and alternatives play an important role in nutrient adequacy. The aims of this study were to quantify the consumption of milk and alternatives within Canadian self-selected diets and determine their contribution to intakes of nutrients and energy. [...] Milk and alternatives contributed >20% to total intakes of calcium (52.62 ± 0.46%), vitamin D (38.53 ± 0.78%), saturated fat (28.84 ± 0.51%), vitamin B12 (27.73 ± 0.57%), vitamin A (26.16 ± 0.58%), phosphorus (24.76 ± 0.35%), and riboflavin (24.43 ± 0.37%), of which milk was the top source. Milk and alternatives contribute substantially to nutrient intakes and thus warrant further attention in terms of mitigating nutrient inadequacy among the Canadian population. https://pubmed.ncbi.nlm.nih.gov/31430962/
-
This is based on rubbish internet misinformation and has no scientific basis. Of course if you have an actual lactose allergy or intolerance you should not consume lactose, just as if you have a peanut allergy you should not eat peanuts. This does not mean all adults and children should avoid eating peanuts.
-
The statement about no CGT being due for share disposals for non-UK residents is correct. No report is necessary to HMRC if you fulfil the residency definitions linked above and do not return to the UK within the time specified. I have disposed of EFTs in this way myself. Note this 5 year absence and non-return period only applies to considerations of CGT. The general definition of a non-resident for tax purposes does not incorporate this 5 year period and is worked out using the UK gov guidelines e.g. https://www.tax.service.gov.uk/guidance/check-your-UK-residence-status/choose-tax-year
- 1 reply
-
- 1
-

-
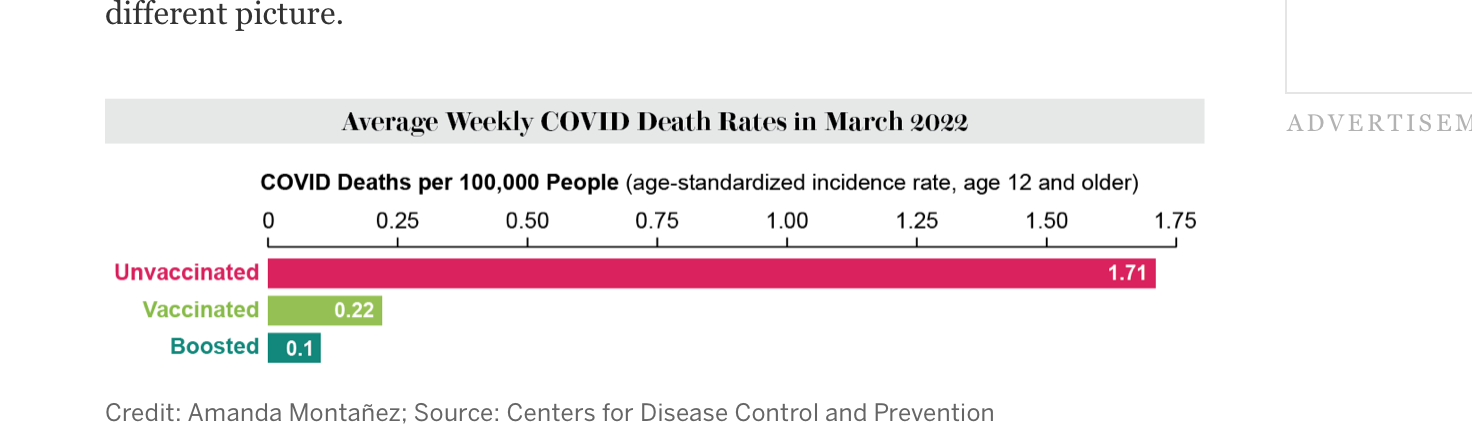
Ineffective is in the eye of the beholder I suppose: https://www.scientificamerican.com/article/how-to-compare-covid-deaths-for-vaccinated-and-unvaccinated-people/
-
Of course they are. Currently about 97% of the US population over 16 has received at least one dose. [https://dig.abclocal.go.com/ccg/interactives/us-vaccine-tracker/vax_us_cdc.html ] If most people are vaccinated and the vaccine has 70% efficacy then 30% of vaccinated people will get the disease and some will die. If 100% of the population have been vaccinated then 100% of people who die of Covid will have been vaccinated. So what. This is self evident.
-
Exactly this was my thought also. A report on TikTok is not a scientifically credible source. It could be completely fictional. If true the condition could be unrelated to the vaccine but assumed by the untrained or predjudiced to be due to the vaccine. There is little to support the truth or accuracy of this account.
-
Antibiotikum (Antibiotiks) for bad cough etc.
partington replied to daviddunham's topic in Health and Medicine
Unfortunately you have completely misunderstood what "antibiotic resistance" means. People do not become resistant to antibiotics - you can neither gain or lose antibiotic resistance as an individual- and this did not happen to you. When physicians and scientists talk about "antibiotic resistance" they mean that the disease causing pathogens -the bacteria- become antibiotic resistant through mutants that survive an antibiotic course. It is the disease pathogen you get infected by that is resistant, not you! Explained simply here: https://www.cdc.gov/antibiotic-use/antibiotic-resistance.html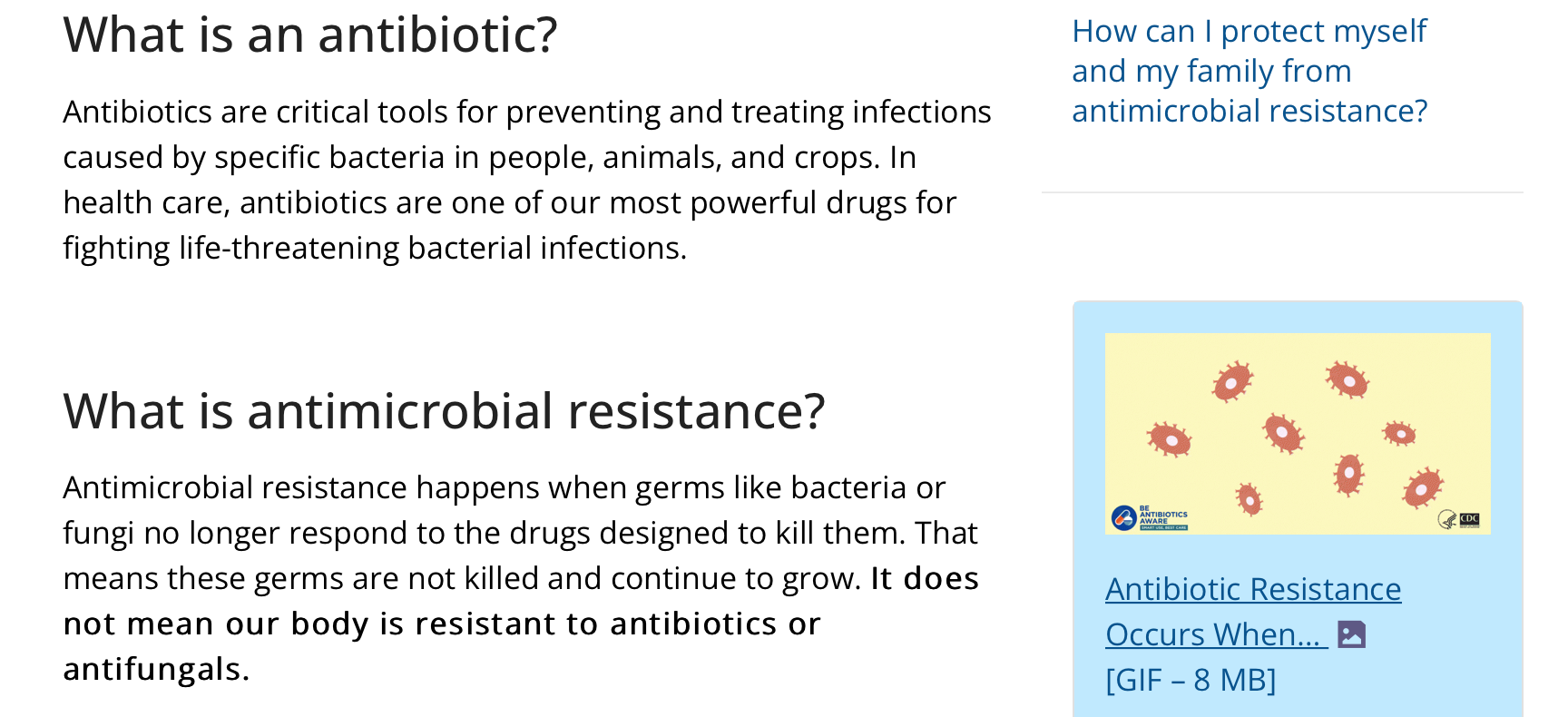
-
Concerns voiced over COVID Deltacron XBC sub-variant
partington replied to webfact's topic in Thailand News
Why do you keep saying this nonsense, when I have literally posted a catalog page showing you can buy a tube of Omicron variant isolated Sars-Cov-2 virus from the European Virus archive, for 2500 euros? Following that link will show you that many other samples of the Covid virus are readily available for purchase too, from the same source. I can only imagine the psychological contortions you will go through trying to deny this definite proof that your claim- that no-one has isolated the Covid virus- is completely absurd. However while you are trying to deny that, here is a completely separate source for the virus. It is the ATCC [American Tissue Type Collection] a US not-for-profit source for cells, viruses, bacteria and other types of biological samples for academic research labs. You will either have to claim this 100 year old world famous reputable bioresearch source[ see second picture below] doesn't exist, or doesn't really have SARS-Cov-2 available for $1,248 a vial! https://www.atcc.org/products/vr-1986hk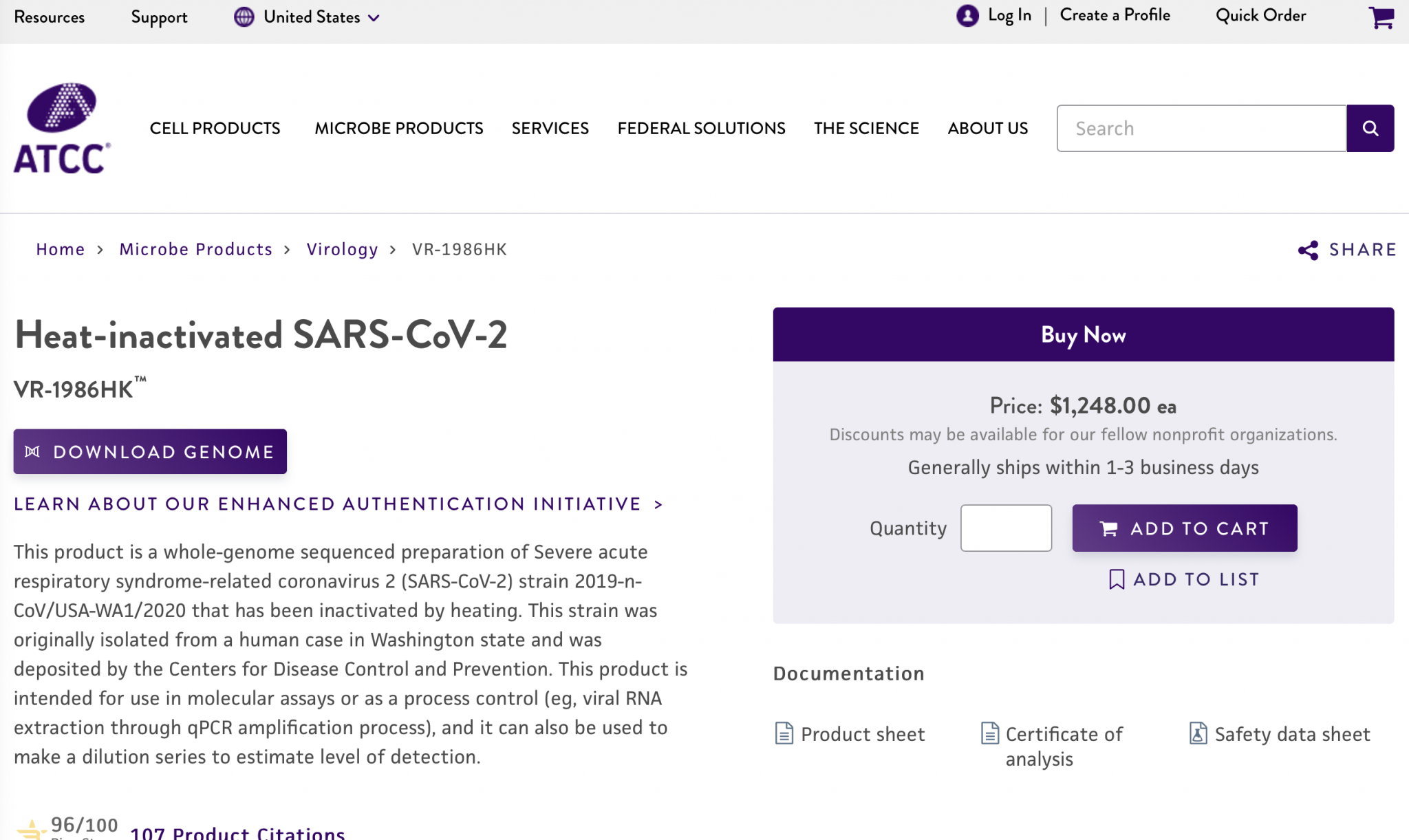
-
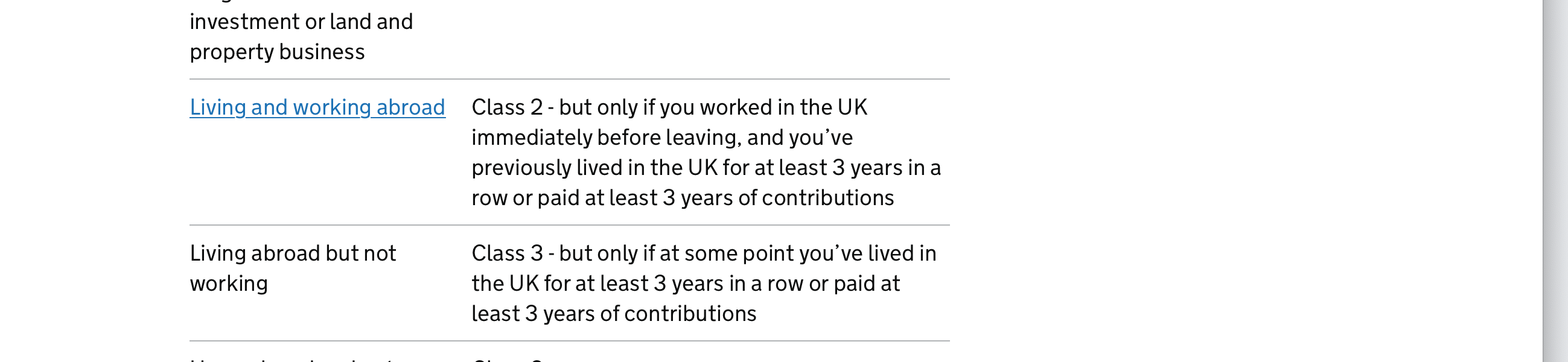
Definitely not true. If you are a man younger than 71 or a woman younger than 69 you can pay for years from 2006 to 2016, but you only have a few months left to do it- until April 2023. Clearly stated here https://www.gov.uk/voluntary-national-insurance-contributions/deadlines
-
Concerns voiced over COVID Deltacron XBC sub-variant
partington replied to webfact's topic in Thailand News
This is complete nonsense. I can't believe how any rational person could accept this fictional narrative. The Chinese Sinovac vaccine is made entirely of isolated Sars-CoV-2 virions. Research labs world wide are able to order Sars-CoV-2 isolates from the same viral isolate banks that store other disease pathogens for research purposes. Here is the catalog page from the European Viral Archive where you could buy a tube of the Omicron variant. Many other isolates are available from the same source, and there are similar banks in the US. Nothing "mainstream" about this. https://www.european-virus-archive.com/virus/sars-cov-2-omicron-ba1-2022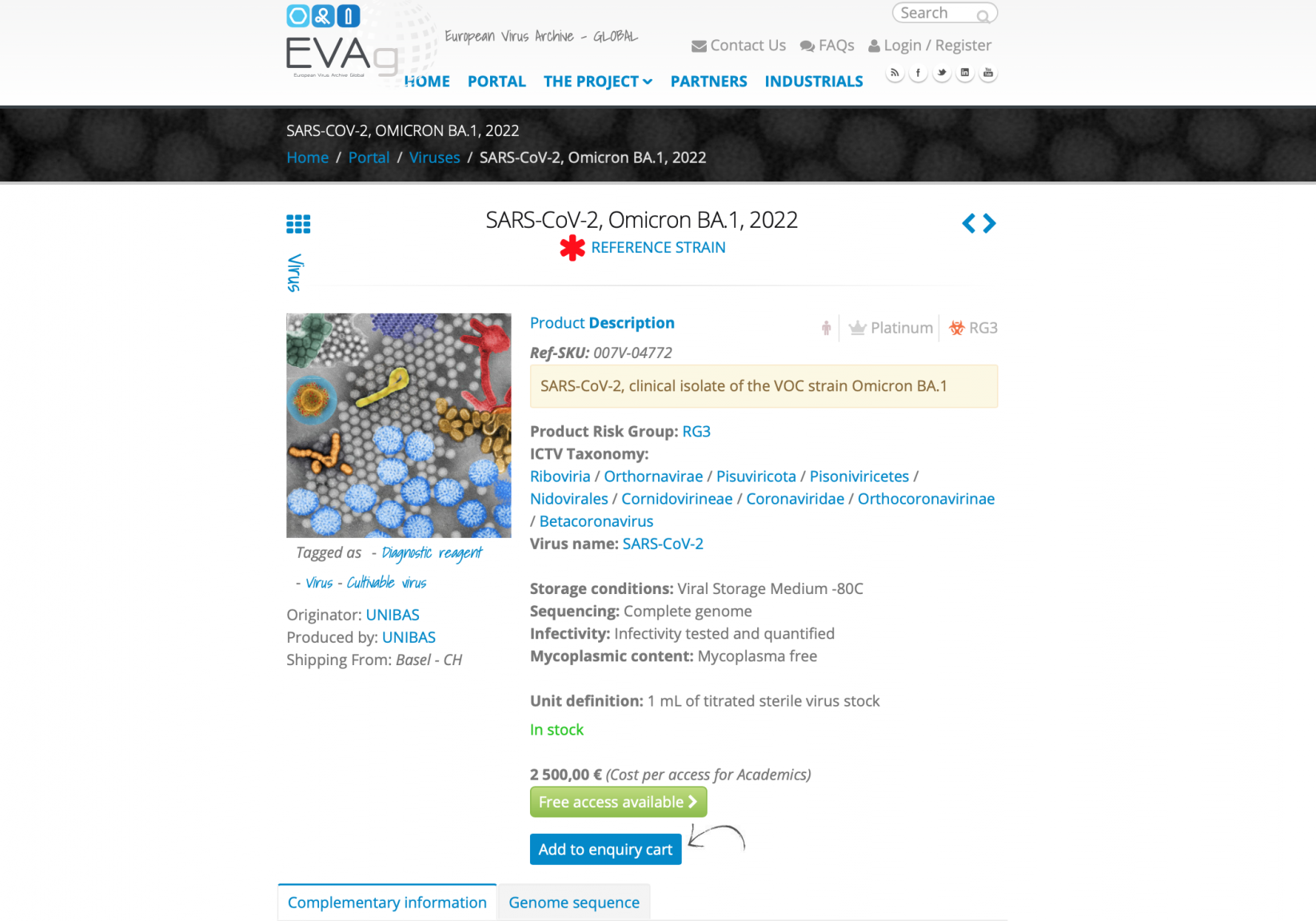
-
What low/medium price wine do you recommend.
partington replied to YorkshireTyke's topic in ASEAN NOW Community Pub
Obviously you are correct and LatPhrao is not, but as a minor cavil, it adds to confusion if you refer to the pre-fermented grape juice as "wine" and then talk about fruit juice being added to "wine"! As I am sure you know, the term for the grape juice (and grape skins for red wine) mix which goes on to be fermented is "must" . I can see why you may be avoiding this usage to avoid puzzling readers, but you could say " pre-fermented grape juice" instead, which takes no longer with cut and paste than typing "wine" which is definitely incorrect. Grape juice isn't wine! I may seem obsessive, but claims that wine is sold as finished wine that then has raw fruit juice added to it have come up again and again in many previous posts. -
What low/medium price wine do you recommend.
partington replied to YorkshireTyke's topic in ASEAN NOW Community Pub
A perennial debate, but one which I still am sceptical about. In my view "fruit wine" is wine fermented from a mixture of grape juice and the juice of other fruits, which are mixed before fermentation starts, and not finished wine made from grapes, to which raw fruit juice is then added before bottling. I think anyone with even moderately functional taste buds could tell if what they are drinking is finished grape wine that has subsequently had raw fruit juice added to it. I could be wrong, of course, but have never seen definitive evidence that convinces me that the raw fruit juice interpretation is true. -
No they aren't. The UK is a representative democracy, not a direct democracy. This means that people vote for MPs who then take independent decisions in government. This is a structure that has evolved to deal with the inescapable truth that most people are ill-informed, prone to short term actions which directly benefit them and not the country as a whole, and lack essential economic, scientific or ethical understanding to adequately determine the best course of action for a country's long term benefit. "At its most basic level, direct democracy means involving the public directly in making decisions. By contrast, representative democracy involves the public choosing representatives, who take these decisions on their behalf. [..] The political thinker Edmund Burke (1729-1797) is one of the most well-known defenders of representative democracy. His view, that elected representatives should not be bound to obey the particular wishes of their electors but should form their own judgements (though be open to hearing and taking into account the views of those on whose behalf they govern), remains influential to this day." https://consoc.org.uk/the-constitution-explained/direct-democracy/
-
Just to make it clear: you are not eligible to pay Class 2 AVCs unless you are living AND working abroad. Because you are retired and presumably neither working or self-employed, you are no longer eligible to continue to pay class 2 contributions, so beware (although the chances of anyone finding out are very low!) Clearly stated here, https://www.gov.uk/voluntary-national-insurance-contributions/who-can-pay-voluntary-contributions and relevant excerpt:
-
Fantastic! Ushers in a welcome era where people who have to choose between heating their home or eating enough will again be told we all have to tighten our belts, but this time by a billionaire. The Tory way. Gotta love 'em!
-
Why do you think the UK being in the EU means "France telling you what to do" but wouldn't involve the UK telling France what to do. Surely both are equally applicable? Why did Belgium, say, or Portugal never complain about the UK "telling them what to do?"
-
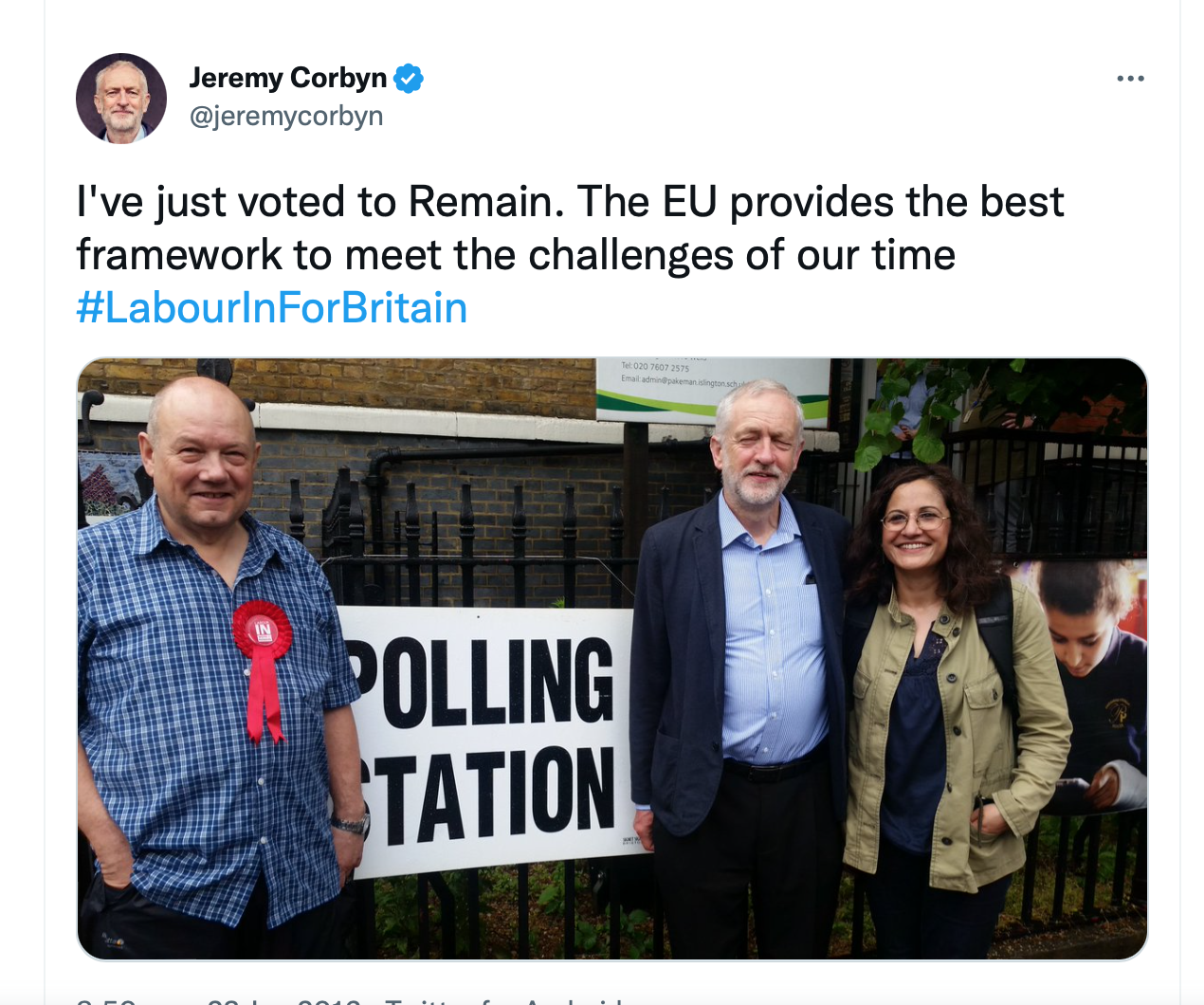
Er... never mind the facts, eh? Corbyn's Twitter in 2016 at the referendum:
-
That's the diagnostic feature of the barely sentient: they don't realise it's a problem. Why? Because they're barely sentient...
-
A "mistake" is knocking over someone's wineglass while reaching for the salt. A series of deliberate lies, deceits and cover ups involving sycophantic cronies reliant on you for a job is intentional wrongdoing, and reveals a personality with no moral anchor or principles. People who want Johnson back, after he was removed because his own party's MPs declared him unfit for office and forced him to leave are, in my opinion, barely sentient.
- 76 replies
-
- 10
-

-

-