.png.3b3332cc2256ad0edbc2fe9404feeef0.png)


TallGuyJohninBKK
-
Posts
35,296 -
Joined
-
Last visited
Content Type
Profiles
Forums
Downloads
Posts posted by TallGuyJohninBKK
-
-

SINGAPORE – As the Covid-19 virus continues to evolve, the Ministry of Health (MOH) and Singapore’s Expert Committee on Immunisation (ECI) continue to recommend an additional dose in 2024 for those who are medically vulnerable. They also encourage all who are aged six months and above to get vaccinated a year after their last dose.
This is in response to a recent study by the NUS Yong Loo Lin School of Medicine (NUS Medicine) and Duke-NUS Medical School, which said the immune response from two doses of mRNA vaccine is enough to protect children against Covid-19 and that a third dose is not needed as it does not extend the benefit.
In an e-mail to the media, MOH said it is aware of a recently published local study but it continues to stand behind the analysis of its own local data... It demonstrated that the protection against hospitalisation in local children increased from 66 per cent with two vaccine doses to 73 per cent with three vaccine doses.
(more)
Looks like Singapore is following a similar COVID vaccine policy to that in the United States, where the CDC has recommended everyone age 6 months and above get vaccinated with the newest XBB-variant COVID vaccine.
-
On 5/8/2024 at 11:32 AM, DonniePeverley said:
We've had it cleaned twice in 6 months ! It's a new condo too.
I've lived in the same rented home in Thailand ever since I moved here many year ago...
Originally, it came with a large and very old floor standing air con in the main kitchen-living room area that literally gulped electric, and didn't do a great job of keeping the living area very cool.
Eventually, after many years, persuaded my landlord to go half-half with us on a large new inverter aircon that does a much better job of cooling.
And, with the change, it's probably shaving a couple thousand baht off our electrical bill most months. Ends up paying for itself in about one year's time.
-
 1
1
-
-
40 minutes ago, BigBruv said:
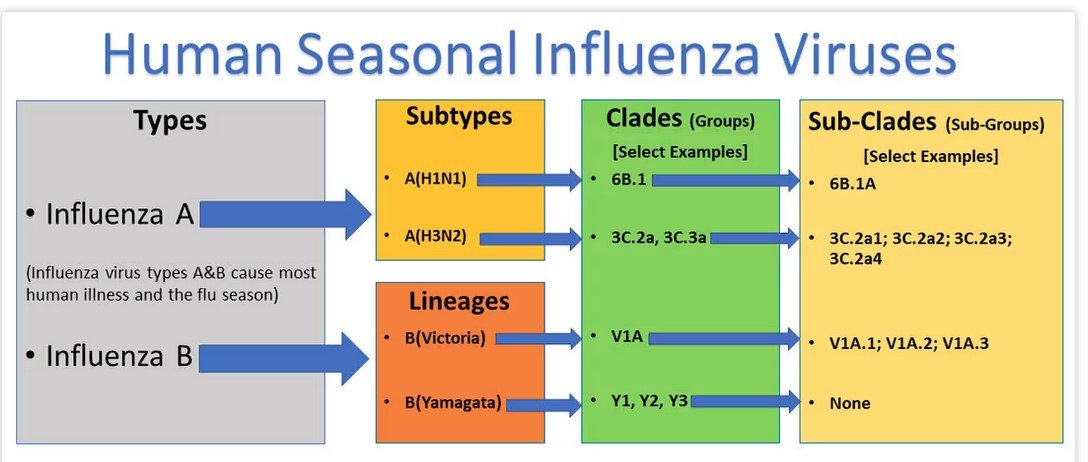
PS. Is there any reason flus aren't given made uup names to market them???
The flu has a lot of different variant names as well, though people may not be as familiar with them.
"There are four types of influenza viruses: A, B, C, and D. Influenza A and B viruses cause seasonal epidemics of disease in people (known as flu season) almost every winter in the United States. Influenza A viruses are the only influenza viruses known to cause flu pandemics (i.e., global epidemics of flu disease).
...
Influenza A viruses are divided into subtypes based on two proteins on the surface of the virus: hemagglutinin (H) and neuraminidase (N). There are 18 different hemagglutinin subtypes and 11 different neuraminidase subtypes (H1 through H18 and N1 through N11, respectively). While more than 130 influenza A subtype combinations have been identified in nature, primarily from wild birds, there are potentially many more influenza A subtype combinations given the propensity for virus “reassortment.”
Live and learn....
https://www.cdc.gov/flu/about/viruses/types.htm
-
1
-
-
21 minutes ago, Woof999 said:
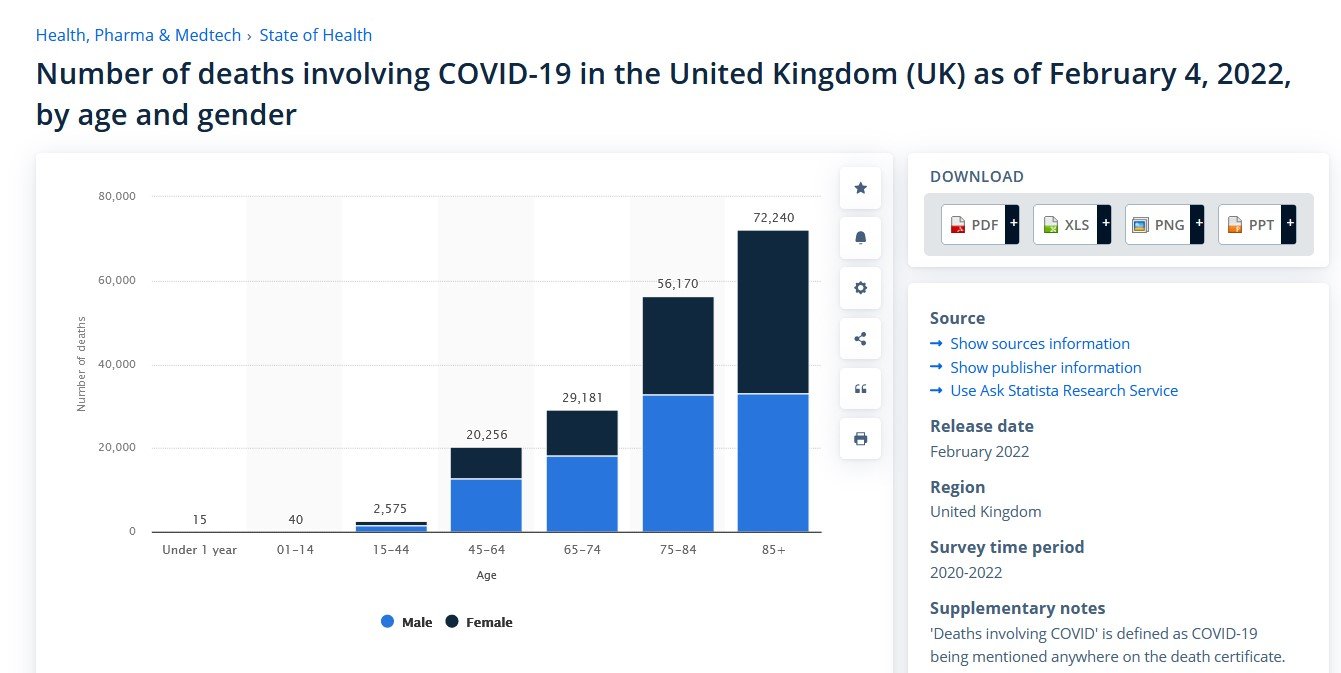
Indeed. I was just highlighting that the percentages shown in the post I quoted looked small but, even when applying only the lowest %age and to the lowest age groups least likely to have underlying conditions, would still equate to many tens of thousands of deaths.
This is UK COVID deaths data by age group for the first two years of the pandemic: The elderly made up the largest share of COVID deaths, but there were sizable deaths as well among several younger age groupings.
https://www.statista.com/statistics/1291744/covid-19-deaths-in-the-united-kingdom-by-age-and-gender/
-
10 minutes ago, Woof999 said:
Let's take just the UK population of 67M and take only those aged between 10 and 39 years old, which I'd estimate at 50%. 67,000,000 * 0.5 * 0.002 = 67,000. 67,000 young people dead in the UK alone, including many with no pre-existing conditions is not to be scoffed at.
The total official death toll from COVID in the UK during the pandemic has been more than 230,000 (all ages) thus far, and growing at about 100+ new COVID deaths per week lately.
https://www.worldometers.info/coronavirus/country/uk/
https://ukhsa-dashboard.data.gov.uk/
-
A bit more background on the latest FLiRT COVID variants, which are not just in Thailand, but many other places as well: -
5 minutes ago, dinsdale said:
No one else does. It's a targeted vaccine within populations.
And Thailand at the national level right now appears to have NO national COVID vaccine policy (unless being absent is a policy).
So, obviously, each country makes their own choices about what they think is best / most affordable / etc.
-
7 minutes ago, Cryingdick said:
The places I was staying in for $100 a night a couple years ago now go for $200 a night. I was looking to book a simple airbnb in Ann Arbor recently, which is midway up to my lake place. A couple years ago I had a decent spot in the center of town for around $100 all in. The last time I looked I couldn't find anything in the center and what was on the fringes was a little over $200.
Yikes!!!
Were there any decent, clean, modest hotel options available there in the $100 to $200 range? I'm thinking there had to have been.
As I mentioned above, I checked out AirBNB and VRBO prior to my U.S. (L.A.) trip last year, and didn't find anything in any area / setting I'd want to stay for anything close to the $100 per night hotel rate I ended up booking.
-
12 minutes ago, dinsdale said:
Why is it that the CDC still says everyone should get the mRNA vax where all other advanced countries don't. Is covid somehow different in the US than say all of Europe, the UK, Aus, NZ etc.
Because the U.S.'s past experience with the level of COVID illness among young people there, sometimes serious, who often haven't been vaccinated, makes them feel that the reward-risk balance favors vaccination.
-
1 minute ago, Cryingdick said:
is it just me or have motels become way worse than I remember them as a kid? I remember when people would go on road trips and vacation in them. Free HBO!!!!!!
the last few motels I have used I refused to undress to sleep on the bed and kept above the blankets. It amazes me also how crackheads seem to pop up even in the most unlikely motel parking lots. More and more they seem to be making trade off the homeless and all that goes with that.
I've noticed the same thing around the L.A. area... The typical motel clientele seems to have taken a big downward turn, and a lot of the properties are old and show little signs of any upkeep and improvements, making them a somewhat sketchy short-term accommodation option.
-
41 minutes ago, Cryingdick said:
I looked at Extended Stay America awhile back and they wanted more than $3,000 a month in some outer burb of Minneapolis. I don't find the value in that
You said you don't find value in that above... e.g. $100 a night in the suburbs... But then you mention that places you consider "pretty decent" are going for $200 per night or higher lately....
I'm not following???
-
38 minutes ago, Cryingdick said:
I looked at Extended Stay America awhile back and they wanted more than $3,000 a month in some outer burb of Minneapolis. I don't find the value in that and it is how I found Airbnb. If Airbnb, Vrbo, don't have it, it doesn't exist.
I was looking today at their (Extended Stay America) properties around the L.A. area, and they typically had nightly rates between $100 and $150, depending on the particular location. However, at least around the L.A. area, a lot of their properties get pretty scuzzy reviews from customers about being dumps... not exactly the business traveler friendly image they try to portray.
Last year when I stayed in L.A., and in other trips, I typically -- with a fair bit of research work -- was able to find some national chain hotels (a Days Inn by Wyndham that I like) that are clean and well kept for around $100 per night. But you have to look.
Of course, if I was going to be there for a full month, that would mean a monthly rate of $3000+ -- which to me seems a crazy monthly price for a small but decent hotel room.
-
10 hours ago, webfact said:
A slight uptick in Covid cases over the past two weeks is deemed expected,
Missed the boat on that one by a long ways:
The weekly COVID new hospitalization counts reported by the MoPH during the past eight weeks have been as follows, with the spring surge beginning well before this year's mid-April Song Kran holidays, but then climbing rapidly after they arrived:
March 16 -- 501
March 23 -- 630
March 30 -- 728
April 6 -- 774
April 13 -- 849
April 20 -- 1,004
April 27 -- 1,672
May 4 -- 1,792
-
1
-
-
1 hour ago, neverere said:
When I asked at the local hospital for one of my daughters, who has only had 2 shots, the nurse told me there was none available and there was no need. For myself, I think just having had Covid should serve as a booster.
The Thai government, at least for the present, seems to have ceased its former practice of offering free and widespread public COVID vaccinations (although I'm not aware that they ever actually announced that change).
However, the latest XBB variant COVID vaccine is available for a fee from at least several locations in Bangkok. Can't speak to the current availability outside of Bangkok.
Here's more info on the BKK availability:
PS -- At least in the West, there is likely to be a new JN.1 or similar variant-focused COVID vaccine available in fall 2024 (later this year). That likely will eventually make its way to the BKK vaccination sources listed above.
But the seasonal peak time for COVID in Thailand typically has been now... March thru June-July... So if anyone has a desire to get vaccinated, now is the right time to go instead of waiting till the fall.
PPS - It's certainly true that the risk from COVID is far greater for older adults, and much less (though not nothing) for young people. The U.S. current policy is everyone should get the newest COVID vaccine. Places like the UK have a different policy to only give new vaccine to the elderly and those otherwise at risk.
-
1
-
 1
1
-
-
23 minutes ago, impulse said:
There are also a lot of extended stay hotels that have monthly room rates.
I was looking at the Extended Stay America chain in the U.S. lately... They claim to advertise monthly rates, and have an extended stay rate for anything longer than 14 days.
However, when I look at their actual rates, they bill those longer stay rates on a single night basis. And when you look at their broader rates, they have several other types of per night rates that are actually lower pricesthan their supposed longer stay rates....
I found nothing where you can actually book one of their rooms by the month -- set price for a full month stay.
-
folks infected with the FLiRT variant are displaying much the same symptoms that were seen with JN.1:
- Fever or chills
- Cough
- Sore throat
- Congestion or runny nose
- Headache
- Muscle aches
- Difficulty breathing
- Fatigue
- New loss of taste or smell
- "Brain fog" (feeling less wakeful and aware)
- Gastrointestinal symptoms (upset stomach, mild diarrhea, vomiting)
https://medicalxpress.com/news/2024-05-covid-variants-flirt.html
-
1
-
4 minutes ago, BigBruv said:
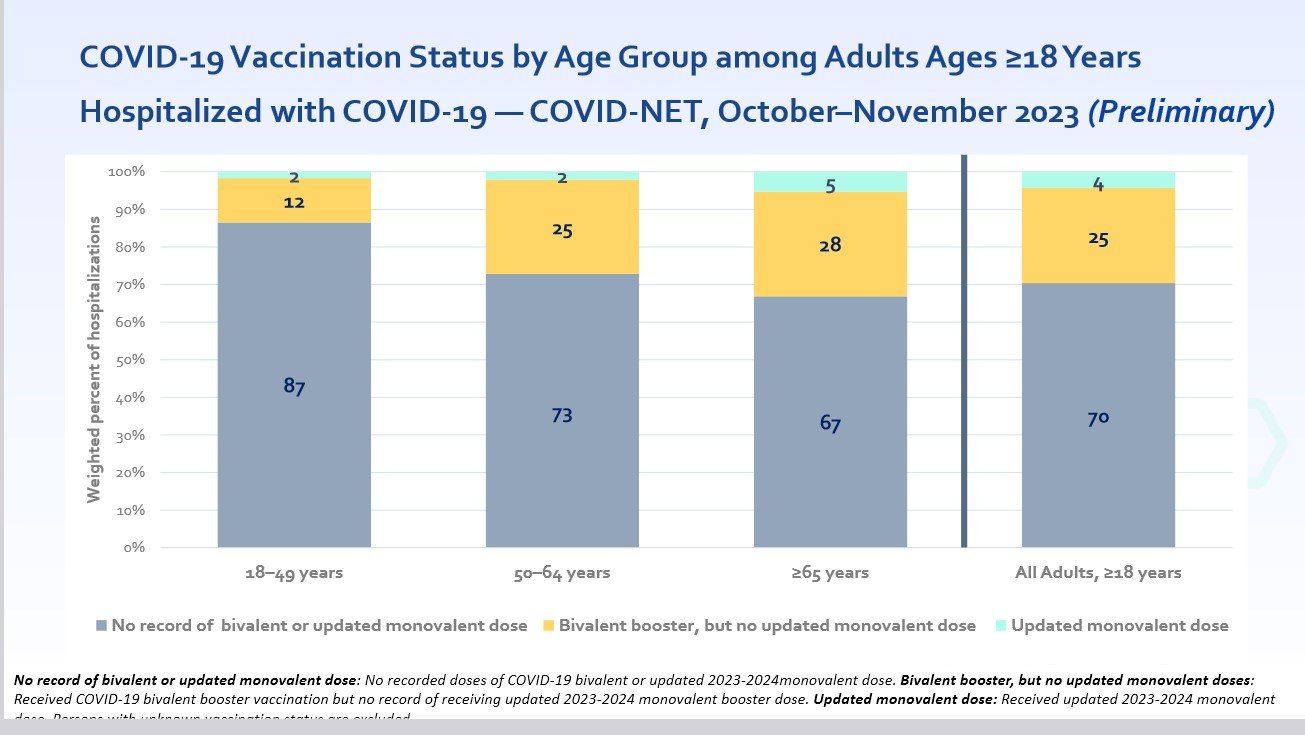
Overwhelming odds are that they would have been *vaccinated on arrival at hospital (if not before)*
Sorry, but that's simply not the way it works in the U.S., where most people have to voluntarily decide if they want to get vaccinated or not.
If it were, the above chart would not be showing what it did, which was 70% of U.S. adult COVID hospitalizations in the subject study were not up-to-date with the recommended COVID vaccinations.
-
For people in the U.S. hospitalized with COVID, the overwhelming odds are they're NOT up-to-date with the recommended COVID vaccines (meaning having received a bivalent booster or the newest XBB monovalent vaccine), per the study below. (the gray shaded columns represent those NOT up-to-date with COVID vaccines:
https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2024-02-28-29/02-COVID-Taylor-508.pdf
Centers for Disease Control and Prevention
National Center for Immunization and Respiratory Diseases
COVID-19–Associated Hospitalizations among
Adults — COVID-NET, 2023–2024 -
2 hours ago, johng said:
Remember this guy on CNN ?

https://www.yahoo.com/news/chris-cuomo-makes-ivermectin-face-210453781.html
Take your pick of the numerous study and public health agency recommendations against the general public use of ivermectin to treat COVID (outside of clinical trials) because it simply hasn't been found to work in credible research.
Yet another study shows little benefit for ivermectin with COVID-19
March 5, 2024A new randomized control trial from the United Kingdom shows that using ivermectin during COVID-19 infections provided little improvement in recovery rates in patients treated in clinics. The study appeared in the Journal of Infection.The anti-parasitic drug has been investigated since 2020 as a potential treatment for COVID-19. Some early trials suggested the drug was able to reduce mortality rates and improve outcomes, but several of them had serious flaws, the authors noted. Subsequent trials and systematic reviews have largely disproved those earlier results...."Overall, these findings, while evidencing a small benefit in symptom duration, do not support the use of ivermectin as treatment for COVID-19 in the community among a largely vaccinated population at the dose and duration we used," the authors wrote.
https://www.cidrap.umn.edu/covid-19/yet-another-study-shows-little-benefit-ivermectin-covid-19
-----------------------------
Ivermectin not effective in treating Covid-19, joint Mahidol-Oxford study shows
February 24, 2023
Ivermectin is not shown to be effective against Covid-19 in clinical trials according to the findings of a joint University of Oxford and Mahidol University study.
The study that was published on the peer-reviewed eLife medical journal found that high doses of the drug ivermectin, controversially recommended by some high-profile political and media figures during the pandemic, is ineffective at treating the virus.
-----------------------------------------
New England Journal of Medicine editorial:Time to Stop Using Ineffective Covid-19 Drugs
Published August 17, 2022
For ivermectin, a meta-analysis of 16 trials8 involving 2407 patients with both severe and nonsevere illness showed no reliable evidence of reductions in mechanical ventilation, hospital admission, duration of hospitalization, clinical severity, or mortality; in addition, the investigators found no effect related to the dose of ivermectin. In light of this available evidence of nonefficacy for ivermectin and fluvoxamine, how much evidence of nonefficacy is enough?
https://www.nejm.org/doi/full/10.1056/NEJMe2209017?query=recirc_curatedRelated_article
---------------------------
2023 WHO Guidelines for treatment of COVID:
WHO updates guidelines on treatments for COVID-19
10 November 2023The update also includes a strong recommendation against the use of ivermectin for patients with non-severe COVID-19. WHO continues to advise that in patients with severe or critical COVID-19, ivermectin should only be used in clinical trials.--------------------------------------European Medicines Agency:EMA advises against the use of ivermectin for the prevention or treatment of COVID-19 outside randomised clinical trials.
In March 2021, EMA found that the published data from laboratory and observational studies, clinical trials and meta-analyses, do not support its use for COVID-19. It therefore concluded that using ivermectin to prevent or treat COVID-19 cannot be recommended outside controlled clinical trials.
-
5 hours ago, Tippaporn said:
Was it peer reviewed? No? How do you treat non-peer reviewed studies performed by those on the other side of you? Do you see a problem? Want to talk about it? Full disclosure?
Sure thing, I'll talk about it (The Royal Society (UK) report on the effectiveness of COVID intervention measures)... Some sources are not typically peer reviewed, because the authors aren't just ordinary individual researchers, such as was the case here... Guess you'll just have to settle for this below (though note below a separate independent review process that did occur with later published summary version of this report).
https://royalsociety.org/about-us/
And from the report itself:
"The Royal Society is a self-governing Fellowship of many
of the world’s most distinguished scientists drawn from all
areas of science, engineering, and medicine. The Society’s
fundamental purpose, as it has been since its foundation
in 1660, is to recognise, promote, and support excellence
in science and to encourage the development and use of
science for the benefit of humanity."Highlights from the report itself:
Masks and enhanced hygiene measures
Published studies generally found that masks
reduced the transmission of SARS-CoV-2,
recognising the risk of bias, and allowing for
uncertain and variable efficacy. Importantly,
there was a ‘gradient of effectiveness’, with
evidence, mainly from studies in healthcare
settings, that higher quality N95/FFP2 masks
were more effective than surgical-type masks.AND
Social distancing and ‘lockdowns’
Most effective of all the NPIs were the
social distancing measures, with a gradient
showing that the most stringent of these had
the strongest effects. Stay-at-home orders,
physical distancing measures, and restrictions
on gathering sizes were repeatedly found to
be associated with significant community-wide
reductions in SARS-CoV-2 transmission, as was
frequently assessed using the time-varying
reproduction number, RtAND
Travel restrictions and controls across
international borders
While most countries implemented some form
of border control, there are a limited number
of studies examining the effectiveness of their
implementation. Based on these, symptomatic
screening widely adopted in the early phases
of the pandemic was found to have had no
meaningful effect on reducing transmission.Apart from the main and original published report, though, it does appear that a later summary version of the above report was published in the Royal Society's own journal with internal peer review, as follows:
Executive Summary to the Royal Society report "COVID-19: examining the effectiveness of non-pharmaceutical interventions"
- August 2023
- Philosophical Transactions A 381(2257):20230211
"This theme issue was put together by the Guest Editor team under supervision from the journal‘s Editorial staff, following the Royal Society‘s ethical codes and best-practice guidelines.
The Guest Editor team invited contributions and handled the review process. Individual Guest Editors were not involved in assessing papers where they had a personal, professional or financial conflict of interest with the authors or the research described. Independent reviewers assessed all papers. Invitation to contribute did not guarantee inclusion."-
1
-
1 hour ago, KhunLA said:
Along with many, harm and injure the recipients, and they get compensated quickly, IF, they know about this program.
... "Total compensation paid over the life of the program is approximately $5 billion"
All of those VICP cases and dollars involve vaccines other than the COVID vaccines, which for now are covered under a different federal program... But nonetheless to add some context on the broader vaccines issue involving VICP:
"How many petitions have been awarded compensation?
According to the CDC, from 2006 to 2021 over 6 billion doses of covered vaccines were distributed in the U.S. For petitions filed in this time period, 10,870 petitions were adjudicated by the Court, and of those 7,846 were compensated. This means for every 1 million doses of vaccine that were distributed, approximately 1 individual was compensated. [emphasis added]https://www.hrsa.gov/sites/default/files/hrsa/vicp/vicp-stats-09-01-23.pdf
"When coverage under the PREP Act Declaration for COVID-19 ends, COVID-19 vaccine injuries could be compensated through VICP, contingent on additional regulatory and statutory changes.
To be included in the VICP, (1) the vaccine must be recommended by the CDC for routine administration to children or pregnant women; (2) the vaccine must be made subject by act of Congress to the excise tax that funds VICP; and (3) the Secretary of HHS must add the vaccine to the Vaccine Injury Table, which lists injuries and conditions associated with vaccines covered by VICP. Should all of these changes occur, COVID-19 vaccines would be covered by VICP.
https://crsreports.congress.gov/product/pdf/R/R46982
-
 1
1
-
-
16 minutes ago, BigBruv said:
The idea that you can catch a RESPIRATORY virus which gives you blood clots is very difficult to believe.
Then I guess you need to bone up on your medical studies:
"It is well established that COVID itself caused a significantly increased risk of these related blood clots and also thrombocytopenia (low platelet count). An August 2021, analysis of 30 million vaccinated people in the UK showed that the risks of thrombocytopenic events were much higher following a COVID infection, compared with any COVID-related vaccine."
https://medicalxpress.com/news/2024-05-astrazeneca-covid-vaccine-withdrawn-victim.html
"Blood clotting is a complex process, involving many different proteins and chemical messengers all interacting with each other in a series of reactions. Venous thromboembolism, an umbrella term for several common blood clotting diseases, is quite common, affecting roughly 17,000 Australians each year. While cases can vary in severity, many are treatable with medications such as heparin and other anti-clotting treatments.
Blood clots are a known complication of COVID-19 itself. One analysis found that 14.7 per cent of COVID-19 patients developed some form of blood clotting, often in places like the legs or lungs, where other blood clots are more commonly found."
Blood clots are also a complication of COVID-19
Researchers have also seen a strong association between blood clots and COVID-19 infection itself, says Hyung Chun, MD, a Yale Medicine cardiologist. “Unfortunately, in those who are sick enough with COVID-19 to be in the intensive care unit [ICU], blood clots have been a major factor in their illness,” Dr. Chun says. Close to 20% of COVID-19 patients in the ICU develop blood clots, he says. “That’s far higher than what you’d expect for patients who are in the ICU for different conditions. Estimates I’ve seen are in the 3 to 10% range for patients admitted for other reasons," adds Dr. Chun.
https://www.yalemedicine.org/news/coronavirus-vaccine-blood-clots
-
1
-
 1
1
-
-
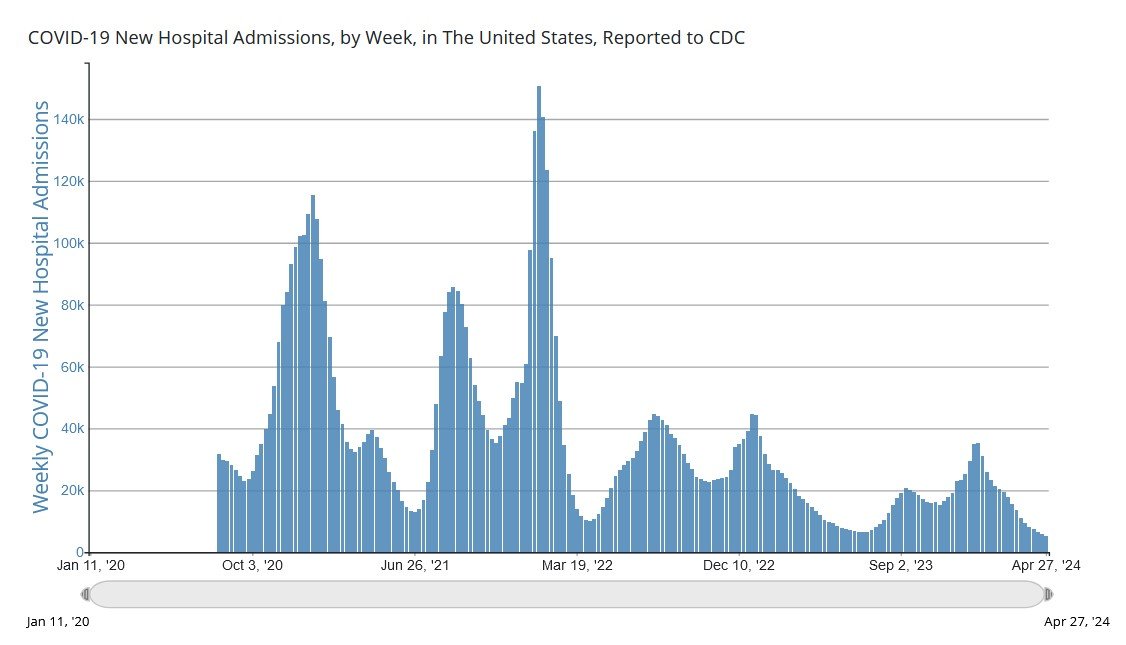
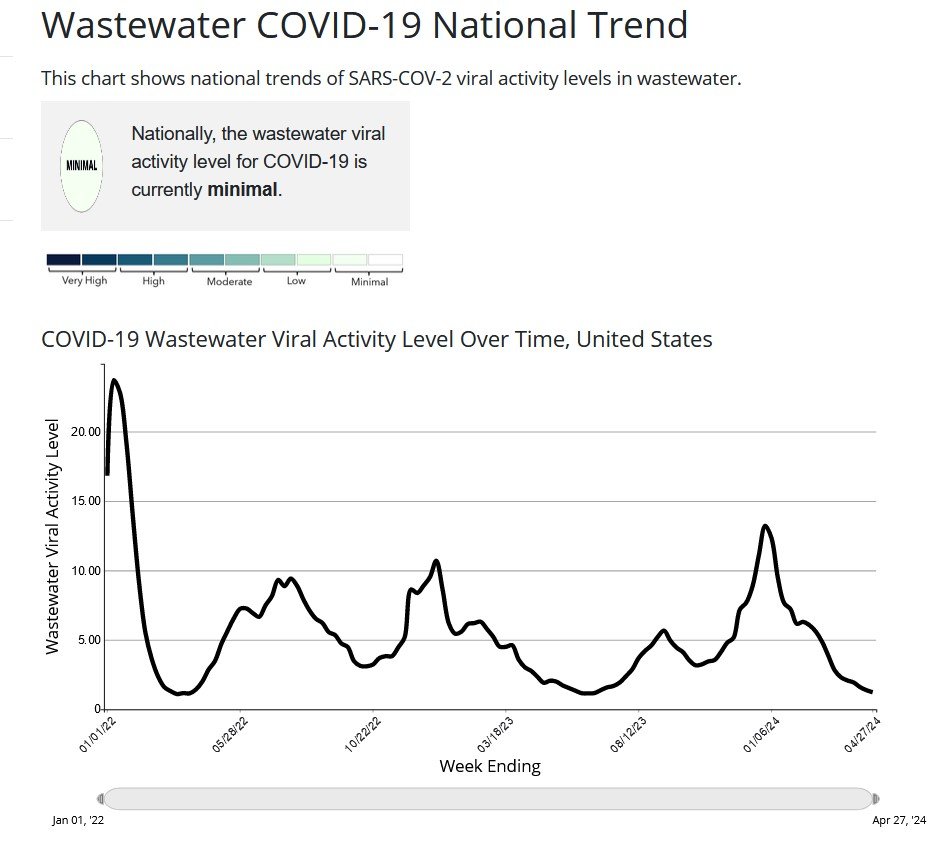
The good news here is, this latest edition of new COVID variants thus far haven't generated any signs of increasing infections or increased hospitalizations in the U.S. The rates for both have been steadily trending down in the U.S., even as the share of the newest variants has been rising compared to their predecessors.
https://covid.cdc.gov/covid-data-tracker/#datatracker-home
https://covid.cdc.gov/covid-data-tracker/#trends_weeklyhospitaladmissions_select_00
https://covid.cdc.gov/covid-data-tracker/#wastewater-surveillance
On the flip side, the potential issues are some initial signs that the newest variants may be more resistant to the current COVID vaccines, and more than three-fourths of the U.S. population haven't even received the most recent XBB variant vaccine rolled out in the U.S. starting last fall, meaning there's potential risks there.
"Speaking to WebMD, Dr. Megan Ranney, dean of the Yale School of Public Health, said the FLiRT variants display some concerning changes. One is alterations in the virus' spike protein, which the virus uses to invade the body and trigger illness.
That type of change worries experts, who point to waning vaccination rates among Americans. Since September 2023, just 22.6% of Americans have gotten themselves an updated 2023-2024 COVID vaccine, the CDC said.
It's possible that even folks who got the latest COVID vaccine aren't well-protected against JN.1 or the FLiRT variants: One preprint study released this week from researchers at Harvard University suggests waning effectiveness against those strains. That study has not been peer-reviewed, however."
https://medicalxpress.com/news/2024-05-covid-variants-flirt.html
-
4 minutes ago, BigBruv said:
The idea that people who died from vaccine induced blood clots & heart attacks etc lived shorter than average fails to appreciate these are the very people who would have been expected to live much much longer - many decades in some cases.
The most famous AZ victim was Lisa Shaw, who was 44 (and left behind a very young daughter)
No one's arguing there were very rare side effects from the AZ vaccine, not even AZ as a general principle. But it will come down to the UK courts to decide whether or not the vaccine was to blame in individual cases, given that both COVID and other medical conditions can and do cause the same kinds of blood clots.
The other thing to keep in context about this is the 50+ plaintiffs in the UK court cases come from among 50 million total AZ vaccine doses given in the UK.... just one indication of just how rare the blood clotting issue has been.
-
1
-


AstraZeneca withdraws Covid-19 vaccine citing low demand
in COVID-19 Coronavirus
Posted
No it doesn't.. And yes, the age of COVID deaths in the UK and elsewhere has been periodically reported, including in posts here on this forum.
But none of that changes the fact that older people who die from COVID, on average, would have otherwise had years left to live, because those who actually survive into their 70s and 80s (absent COVID) have longer life expectancies on average than the overall population averages at large.
But, it is a common claim that COVID deniers make it order to falsely minimize the impact of the pandemic.
Average Covid-19 victim dies years before they otherwise would
What was claimed
The average age of Covid-19 deaths is higher than the average life expectancy, which means that people who get Covid live longer.
Our verdict
This isn’t how life expectancy works. Life expectancy is an average, pulled down by people who die young. As you age, your life expectancy increases. People dying from Covid-19 lose about a decade of life on average.
https://fullfact.org/news/boris-johnson-whatsapp-covid-life-expectancy-cummings/