cmarshall
-
Posts
2,464 -
Joined
-
Last visited
Content Type
Profiles
Forums
Downloads
Everything posted by cmarshall
-
Although like a lot of us I tend to blame those people for bringing death upon themselves, but they are also victims of the right-wing scam. Remember when the Republicans were going on about "death panels" which they imagined in Obamacare. That was before they decide to convert their followers into lemmings.
- 169 replies
-
- 11
-

-

-
-
Book Banning in the Southern USA
cmarshall replied to seedy's topic in US & Canada Topics and Events
I have always thought that Lincoln made a big mistake in not letting the Slave States secede. -
It is the height of foolishness to buy a place in a country where you do not have the right to live.
-
How Japan succeeded in controlling Covid
cmarshall replied to cmarshall's topic in COVID-19 Coronavirus
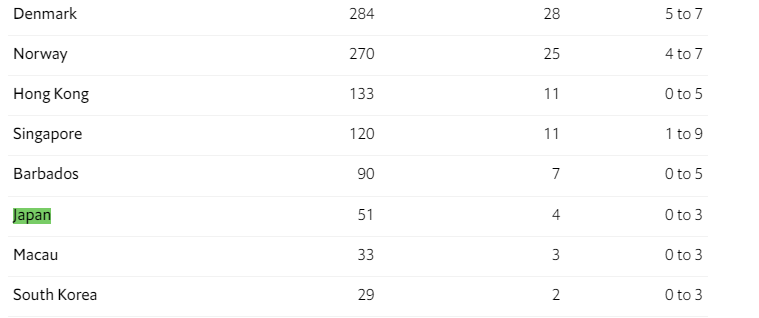
While it's true that Omicron is more infectious its transmission vector is the same as it always was: aerosols. So, the methods that have reduced transmission to date will still work, although they might be applied with more stringency. Japan, as you can see from the data, is doing just fine as are S. Korea, Taiwan, and other countries with effective governments. In the coming months if Omicron infection diminish as expected Japan will reopen. If not, they won't. -
How Japan succeeded in controlling Covid
cmarshall replied to cmarshall's topic in COVID-19 Coronavirus
That was the argument in 2020 of Dr. Tegnel and Giesecke in Sweden, that in the end all countries would have the same infection and mortality rates so it was futile to attempt to resist widespread infection. It certainly hasn't turned out that way and Tegnel and Giesecke are medical crackpots in my opinion who ought to be in prison by now. The countries that have controlled Covid effectively for the past two years are continuing to do so with the Omicron variant as these up-to-date numbers from "The Economist" show. The column on the right is the number of Covid deaths per hundred thousand: https://www.economist.com/graphic-detail/coronavirus-excess-deaths-estimates
-
How Japan succeeded in controlling Covid
cmarshall replied to cmarshall's topic in COVID-19 Coronavirus
Shutting the borders was never going to be enough, because borders are leaky, but stopping travel from China did give a head start on the range of control measures to the countries that took that step. It would be silly to dismiss as irrelevant the strict local lockdowns that countries like China and Australia imposed and which we know stop transmission in those areas. Similarly, Viet Nam has a good record in controlling Covid by conducting the most extensive contact tracing program of any country as well as local lockdowns. But the overwhelming factor in whether a country succeeded in controlling Covid was whether the government ever really tried to do so. The UK, US, and Swedish governments pointedly did not try to stop Covid. The Asian governments, all of which were strikingly successful by comparison with Europe and the US, did make vigorous efforts to stop Covid. I am puzzled that the posters here search and search for some other explanation than the obvious one. -
How Japan succeeded in controlling Covid
cmarshall replied to cmarshall's topic in COVID-19 Coronavirus
Far too simplistic. According to the Global Obesity Observatory, the US is the 14th most obese nation, but the first thirteen are Pacific island nations with tiny populations. So, among highly populous nations the US is the most obese. That might possibly explain the very high rate of US Covid deaths per hundred thousand at 264, but for the fact that Australia and New Zealand are not far behind the US in obesity (18th and 19th respectively,) but they had far lower Covid death rates than the US at 12 and 1 per hundred thousand respectively. https://data.worldobesity.org/rankings/ -
How Japan succeeded in controlling Covid
cmarshall replied to cmarshall's topic in COVID-19 Coronavirus
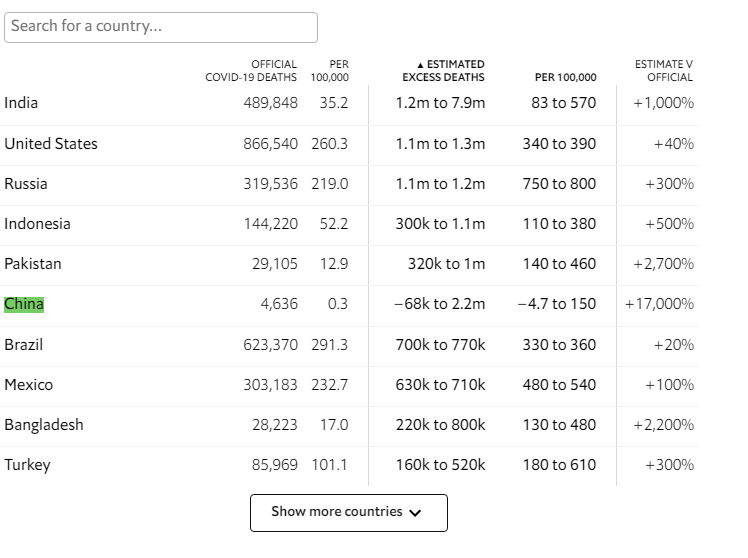
It's not true that we have no idea how well China managed Covid. For example, "The Economist" maintains estimates of excess deaths that includes China. From the table below you can see that the estimate of Covid deaths for China using the excess deaths method is much higher than the official count, as is also true for the US, but even the higher estimate puts China at a level comparable to the European countries and about half of the real US Covid death rate. On the other hand, if you prefer to believe that there is no data at all for anything about China leaving only your prejudices on which to base your opinion, you are welcome to do so. https://www.economist.com/graphic-detail/coronavirus-excess-deaths-estimates
-
How Japan succeeded in controlling Covid
cmarshall replied to cmarshall's topic in COVID-19 Coronavirus
China reported growth of 8.1% in 2021, although it had slowed down by the fourth quarter. That seems reasonable in view of the fact that the reduction in consumer spending on services in the US and elsewhere was accompanied by an increase in spending on goods, to the benefit of both China and US retailers like Amazon.com, etc. Also, China managed the epidemic very well without ever having a national lockdown. -
How Japan succeeded in controlling Covid
cmarshall replied to cmarshall's topic in COVID-19 Coronavirus
Not taboo, but irrelevant without any data to support its importance. -
How Japan succeeded in controlling Covid
cmarshall replied to cmarshall's topic in COVID-19 Coronavirus
Yes, a factor, but not the main factor which, as Dr. O<deleted>ani points out, was that the Japanese virologists were better at the science than in the West and the government listened to them. -
How Japan succeeded in controlling Covid
cmarshall replied to cmarshall's topic in COVID-19 Coronavirus
*Deleted post edited out* By this late date you still haven't caught on to the excess death method of estimating the true Covid death rate which fully accounts for your by now quite out-of-date objection? https://www.economist.com/graphic-detail/coronavirus-excess-deaths-estimates -
How Japan succeeded in keeping its Covid death rate of 14.66 deaths per hundred thousand so low has been a mystery. Some people suspected that the Japanese were simply under-reporting or that they benefitted from some lucky environmental factor like climate. Japan never locked down although they did ban entry by foreigners. Here is a link to an article in today's New York Times by Dr. Hitoshi Oshitani, a virologist, who advised the Japanese government on Covid policy. His explanation is that he and his colleagues determined as early as February, 2020 that aerosol transmission from asymptomatic carriers was the likely vector of infection. They then decided on a novel approach to contact tracing which was retrospective contact tracing, rather than the prospective method applied elsewhere when contact tracing was attempted at all. Instead of trying to identify all the persons who had contact with someone after he became infected, they traced back the contacts that the infected person had previously to try to identify who it was who infected him. This was a plausible strategy only because they Japanese scientists had also figured out that most of the spread of Covid occurred indoors and was due to a limited number of superspreaders, i.e. infected persons who spread much more virus than the average infected person. This retrospective method offered one huge advantage in that the number of contacts to be traced did not explode exponentially as happens with the prospective method to the point of overwhelming the tracing strategy altogether. To those familiar with economics this brings to mind the Pareto Rule in which 80% of an outcome is due to only 20% of the participants. So, Warren Buffet's outstanding investment record over the decades is due to a very small number of investments that vastly outperformed while his average investments only performed to an average outcome. Similary, Amazon has studied the returns for refunds of their products, which are a significant expense, and found them to be due to 20% of their customers. That's why if you return their products a little too often they will close your account. In addition to identifying the superspreaders Dr. Oshitani and his colleagues also recognized early that spreading occurred indoors in a limited number of settings such as restaurants, bars, gyms, etc. The government therefore adopted and consistently promoted a message to avoid the "Three C's," i.e. closed spaces, crowded spaces, and close contact settings. The Japanese people cooperated because they trusted their government. So, very impressive. By contrast in 2020 medical crackpots like Drs. Tegnel and Giesecke in Sweden were putting into effect the bogus "herd-immunity" strategy of simply doing nothing. This was a policy that lacked any basis in science and condemned vulnerable populations, such as nursing home residents, to high mortality rates since the Swedish government took no steps at all to protect them. It's hard to miss the message that both rich and poor Asian countries as a group far outperformed Europe and the US in protecting their populations. The US count of Covid deaths per hundred thousand is currently at 264. https://www.nytimes.com/2022/01/24/opinion/japan-covid.html
-
That's true, but if you were to watch the video whose link I posted, you would hear that doctor point out that the widespread failure to follow the best practices recommended by the medical standards committee that he references has resulted in overtreatment.
-
Well, there ought to be a lot of data to support your assertion since I remember one large scale study of diagnoses and outcomes in the US that found that 40% of cases were misdiagnosed. One of the aspects of living in the Thailand that I enjoy the most is being out of the clutches of the American medical system.
-
This argument reminds me of the arguments of the Brexiteers in the UK for whom it seemed like a good deal to shave 4% off their annual GDP every year in order to gain that will-o'-the-wisp "sovereignty."
-
While you have been lulling yourself to sleep at night with the appealing prospect of one day bringing a medical malpractice suit, the doctors have been investing their more than adequate incomes in tort reform with the result that The results showed that 55% of all medical malpractice claims involved litigation. Of the cases that resulted in litigation, 54% were dismissed by the court in favor of the medical provider. Of the cases that were not dismissed by the court, between 33 and 50% were settled before they reached a trial verdict. Only 4.5% of medical malpractice claims reached a trial verdict. What’s more, of the few cases that did reach a verdict, right at 80% resulted in favor of the medical care specialist. https://www.collinsattorneys.com/medical-malpractice-attorney-albuquerque/common-medical-malpractice-claims/medical-malpractice-claims-litigation-and-trial-numbers/
-
So you believe, but what you really get is defensive medicine designed not to provide you the best care, but to protect the doctor from your lawsuit, which means more than merely excessive testing. I have personally experienced the disadvantages of that system when my New York doctor made it pretty clear that he wanted me to take a medicine that had already caused me serious, painful side effects, because the standard treatments protected him from some possible future lawsuit by my widow. I feel that I got the best standard of treatment from the best doctors at a bargain price which is a better assurance than the opportunity to bring a lawsuit. Just as an aside, the fact that my wife could stay with me in the room was an immense benefit that would not have been available to me in the USA.
-
Where did you get the idea that medical treatment in the USA, for example, comes with a warranty?
-
How do you figure that? I got inpatient care, with correspondingly greater risk management, at a price that matched the lowest in the US, which would be for outpatient treatment. Sounds like a bargain to me. So, you would fly back to the US for such treatment? Why on earth would anyone do that? Why would anyone maintain health insurance in the US while living in Thailand, beyond the minimum Medicare parts A & B?
-
So far, I would recommend laparoscopic. The healing progresses by the hour. I would ask the prospective surgeon how many such operations he has done in the past year. The only advantage I see for open surgery over laparoscopic is that only a local anesthetic is needed. In all other respects laparoscopic seems to be superior.
-
Same here. I have been using an Omron for years. As the doctor in the video I posted explained home measurements are usually lower than in the doctor's office. White coat explains part of it, but another part is that office measurements are often not taken correctly which results is higher readouts and corresponding over treatment.
-
Chula has the reputation of having the best doctors in Thailand. My surgeon certainly inspired my confidence.
-
I hope none of my neighbors in my building are DIY electricians.
-
So, I just had laparoscopic inguinal hernia repair. I decided to have it done at Chulalongkorn Hospital's after hours clinic, with the expectation that it would cost somewhat more than at the daytime clinic, but with less waiting. The operation went as expected without any problems so far. What is kind of interesting is the payment system. I made every effort to identify all the costs up front, but apparently pricing for health care services in Thailand are as opaque as in the US. When I asked the surgeon what it would cost he said THB 130,000. Immediately afterward in the scheduling discussion, the nurse quoted me THB 164,000 to 174,000 not counting the room for overnight stay for which she would not have a quote until the day of the operation since it depended on availability. Some rooms go for THB 30,000 per night and if that turned out to be all that was available we would be stuck with that unless we rescheduled which I wouldn't have done. So, when we called on op day for the room quote she said THB 4500, which was fine. Stayed one night and could move around with minimal discomfort the next day, so staying a second night was not necessary. The bill I was handed was THB 131,000 all in. There was also a pre-op checkup a few days prior which cost THB 1900, a Covid PCR test the day before at THB 1300, and the initial consultation at THB 1000. Turns out the room she quoted for THB 4500 came in at only THB 3500. An internet search of the US cost of laparoscopic inguinal hernia repair showed a range of $3900 to $12,500 with an average of $7,750. I especially enjoyed the experience of getting Thai medical care along with Thai people and would recommend it. I did note that when applying for my patient card at Chula they did not accept my US passport card, but insisted on seeing my US passport book which they checked for a valid visa. On subsequent visits when they requested my passport I always gave them my US passport card, which they did accept. One curious observation. Thai staff apparently do not know how to measure blood pressure correctly. Neither can the fully automatic BP machines in use there. You can find out how it should be done in this lecture by a specialist who references the research. It is worth pointing out that in the US many people including doctors who take BP readings are not using best practices either. I fired one doctor in New York for asking me questions while he was taking my BP.