GroveHillWanderer
-
Posts
4,008 -
Joined
-
Last visited
Content Type
Events
Forums
Downloads
Quizzes
Gallery
Blogs
Everything posted by GroveHillWanderer
-
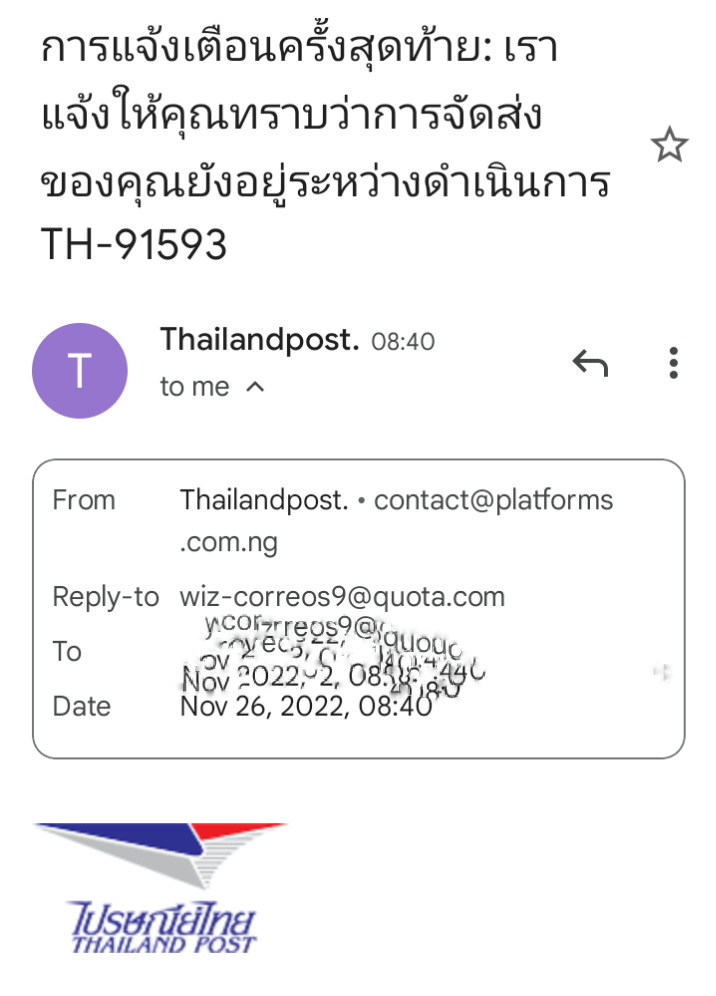
Just "a word to the wise" as the saying goes - there are some emails going round that purport to be from Thailand Post, talking about a payment that is needed for delivery of a parcel, and that ask you to click on a link in the email. A closer look at the details of the sender shows that the email is from an address in Nigeria (.ng suffix) so is highly unlikely to be genuine. See example below where the full email address is visible (it usually isn't, unless you click to reveal it).

-
You must be disappointed then. ????
-
If you mean the Thai channels, @norfolkandchanceposted a graphic earlier in the thread showing those. The original of that is on the Pattaya News site but I'm not sure whether a link is permitted under forum rules.
-
According to the online schedule, the England game tonight is on True Sports 2 & True 4U, in addition to any other Thai channels it may be on. Not sure if TS2 is free-to-air for everyone, but I think T4U is.
-
I'm actually finding it on 3 TrueVisions channels: True Sports 2, True4U and T Sports 7. Channel numbers 606, 024 & 007 respectively.
-
According to reports on the BBC and elsewhere, Twitter has now effectively closed down its premises. All its offices are shuttered. Twitter locks staff out of offices Supposedly this is only a temporary closure but who knows?
-
PayPal no longer available to foreigners in Thailand
GroveHillWanderer replied to webfact's topic in Thailand News
It depends if you're a Thai national or not. You have to be enrolled in the Thai NDID system and if you're not a Thai citizen, you can't enroll. -
Govt: Thailand to Become International Hub of Electric Vehicles
GroveHillWanderer replied to webfact's topic in Thailand News
700 km may be pushing it a little - BMW's official figures say 623 km WLTP range. Although on the NEDC scale, that would probably be close to 700 km. BMW i7 highlights It's true that if you had to replace an entire EV battery all at once, that would indeed be an expensive proposition. However that's a situation unlikely to face many EV owners. Current estimates of EV battery life are about 20 years, which is way more than the average ownership of most motor vehicles. Even after that, only some cells would normally need replacing, not the whole battery. And as the technology improves, battery life will only get better. Tesla is currently developing an EV battery that will last for a million miles, which they say they are close to achieving. -
Fairly sure he means, "tampered with." Although why someone would suspect a financial institution of tampering with their note-counting equipment, I'm not sure. Since in my experience, they usually use the same machines to count the money they're receiving, it would be somewhat counter-productive for them to deliberately mis-calibrate them.
-
As the article clearly states: "While online payment services for utilities are currently available in many locations throughout Thailand, this isn’t the case in Hua Hin, or at least for people who are billed from the Hua Hin Municipal Waterworks Division."
-
I haven't actually tried to use it for a while but as far as I can tell, existing K online cards should still work. When I look up my online (virtual) card details I see the following message:
-
Electric plane manufacturer takes off, receives worldwide orders
GroveHillWanderer replied to Scott's topic in World News
Looking at the figures in the article quoted by @billd766 it sounds economically viable. "Based on U.S. industrial electricity prices, the direct operating cost with nine passengers and two crew, flying at 240 kn (440 km/h), is claimed to be $200 per hour, which compares to $600–1,000 per hour for existing aircraft of similar purchase price such as the Cessna 402s, Pilatus PC-12 and Beechcraft King Air, for operations on routes under 500 nmi (930 km)." -
You didn't notice any authoritarian moves by Trump? Were you hiding under a rock during his presidency? As for examples, try the ones in the articles below: Trump's use of the authoritarian playbook Trump is an authoritarian Trump’s Moves Are Right Out of the Authoritarian Playbook Trump made two remarkably authoritarian remarks in one day The authoritarian moves listed there include (but are not limited to) sending paramilitary forces from the Department of Homeland Security to quell nonviolent protests, celebrating the wounding of a journalist by police as “a beautiful sight,” spending an election year casting doubt on the legitimacy of the electoral system, calling independent journalists, "the enemies of the people," attacking and calling for the removal of judges whose decisions he didn't like and calling his main political opponent an "enemy of the state." As pointed out in those articles, all of these things are classic examples of authoritarian moves.
-
Electric plane manufacturer takes off, receives worldwide orders
GroveHillWanderer replied to Scott's topic in World News
True, as pointed out in @billd766's post, this aircraft carries "nine passengers and two crew" and as the quoted article further states, "55% of airline flights [...] fall within its 565 nmi (1,050 km) range ..." So it definitely isn't intended to replace conventional aircraft on long-haul routes but it could probably handle a decent number of commuter routes that represent a large proportion of flights. -
Electric plane manufacturer takes off, receives worldwide orders
GroveHillWanderer replied to Scott's topic in World News
These wind turbines were 20 years old, inefficient and at the end of their working life. As mentioned in the article below, they were due to be decommissioned no matter what was going on with the lignite mine. German windfarm to be dismantled -
British man sentenced for rape in UK flees to Thailand
GroveHillWanderer replied to webfact's topic in Thailand News
They don't know for sure. All they say is that "Police enquiries suggest he has fled [...] to Thailand." -
Based on what current trend or development?
-
The way it's worded implies the person in question has a choice of whether to iron a shirt or not. He doesn't.
-
Citrus Extract Spray Prevents Covid, influenza
GroveHillWanderer replied to snoop1130's topic in Thailand News
There were a number of vaccines being developed by Thai researchers (at least 3 that I can recall, though there are probably more). As far as I know research efforts are still ongoing but none of them have completed phase 3 clinical trials yet. -
They still are. BBC and ITV are sharing the coverage between them. Live World Cup Football on UK TV
-
PayPal no longer available to foreigners in Thailand
GroveHillWanderer replied to webfact's topic in Thailand News
Full verification to use Paypal Thailand going forward certainly does need more than just a 13 digit number. As several people have already pointed out, it requires you to be registered with the NDID system. You can do this with your online banking app or by going to your bank branch but in either case, to be accepted into the NDID system it requires a Thai national ID issued to a Thai citizen only. -
I'm sure Blatter would love it if you paid him a bung but I don't think it would do much to help, since he has been banned from any involvement in FIFA activities since 2015.
- 109 replies
-
- 10
-

-

-
It doesn't say decisions will be made in three minutes, it says that the application time will be three minutes. They're talking about how long it takes to submit the application online, not how long it takes to be approved.
-
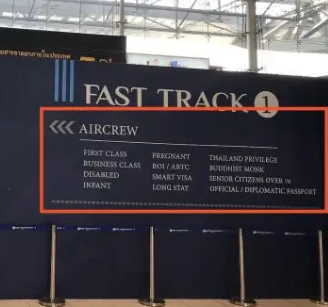
There are a number of different categories of people who can use the Fast Track lane, including if you're over 70 years old, according to the signs at the airport.